Sleep & Rest.
5 peptides, ranked.
Sleep & Rest is the Blueprint layer for understanding why sleep fails: onset, maintenance, quality, circadian timing, stress, pain, reflux, apnea, medications, caffeine, alcohol, and recovery. It starts with foundation and red flags before any peptide discussion. Each candidate was evaluated against your BioProfile, training load, and declared contraindications. The strongest matches sit at the top; secondary options remain visible for comparison.
Sleep foundation - before peptides
Sleep & Rest is not about finding a sedative. It starts by identifying which part of sleep is breaking: onset, maintenance, quality, circadian timing, stress, pain, apnea, medications, caffeine, alcohol, or recovery. The compounds below are analyzed as sleep and rest mechanism education, not as substitutes for sleep evaluation, CBT-I, apnea treatment, medication review, or medical care.
- Regular sleep and wake timing, including weekends and travel recovery days.
- Morning light, evening light exposure, screen timing, room temperature, and wind-down routine.
- Caffeine amount and timing, alcohol pattern, late meals, reflux triggers, and nighttime hydration tradeoffs.
- Stress, anxiety, HPA-axis load, rumination, and the difference between calming arousal and sedating the body.
- Pain, tendon irritation, gut discomfort, reflux, overtraining, and recovery debt that fragment sleep.
- Snoring, witnessed pauses, daytime sleepiness, suspected apnea, restless legs, parasomnias, and medication changes.
- CBT-I, sleep diary, wearable data when available, and the difference between sleep duration and restorative sleep quality.
Sleep red flags - when this is not a peptide question
Some sleep patterns should be investigated before peptide matching. This section is intentionally educational rather than alarmist: in these cases, sleep medicine, primary care, mental-health care, medication review, or urgent evaluation can matter more than any peptide comparison.
- Loud snoring with witnessed breathing pauses, choking, morning headaches, or strong suspicion of untreated sleep apnea.
- Severe daytime sleepiness, falling asleep while driving, sleep attacks, suspected narcolepsy, or occupational safety risk from shift work or jet lag.
- Chronic insomnia 3 or more nights per week for 3 or more months, especially when function is impaired.
- Restless legs, dangerous parasomnias, recurrent nightmares with safety risk, severe depression, or suicidal ideation.
- Chest pain, shortness of breath, severe reflux, intense pain, or sudden sleep worsening after a medication change.
- Heavy alcohol or sedative use, chronic benzodiazepine or Z-drug use, or multiple sleep medications without review.
- Persistent non-restorative sleep despite enough hours, especially with apnea, endocrine, mood, pain, or inflammatory context.
Ranked list
| Rank | Peptide | Match | Evidence | Regimen | |
|---|---|---|---|---|---|
| 01 | 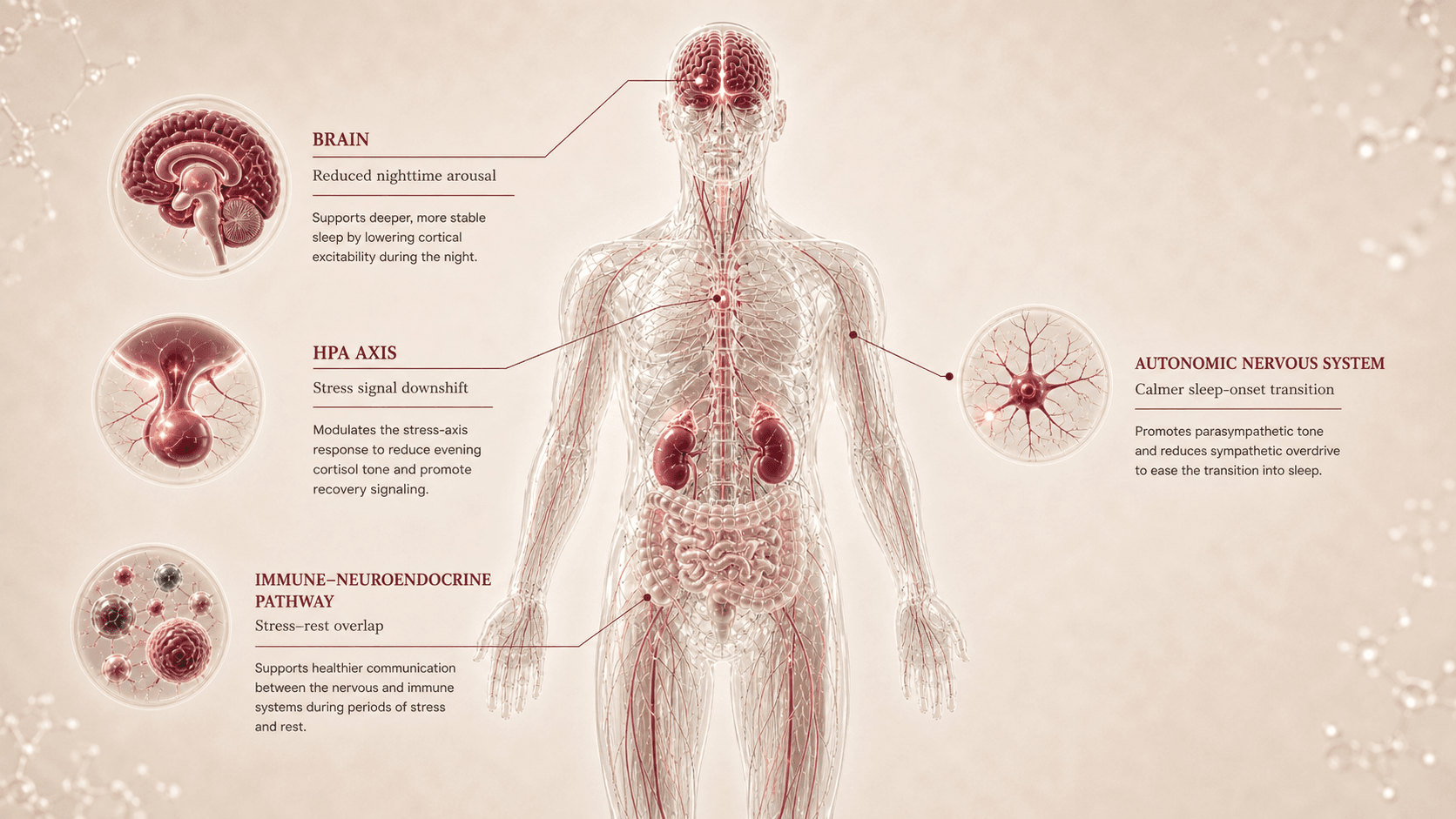 Selank tp-7 - selank acetate | 86 | xCresearch only | intranasal - no protocol timeline | View |
| 02 | 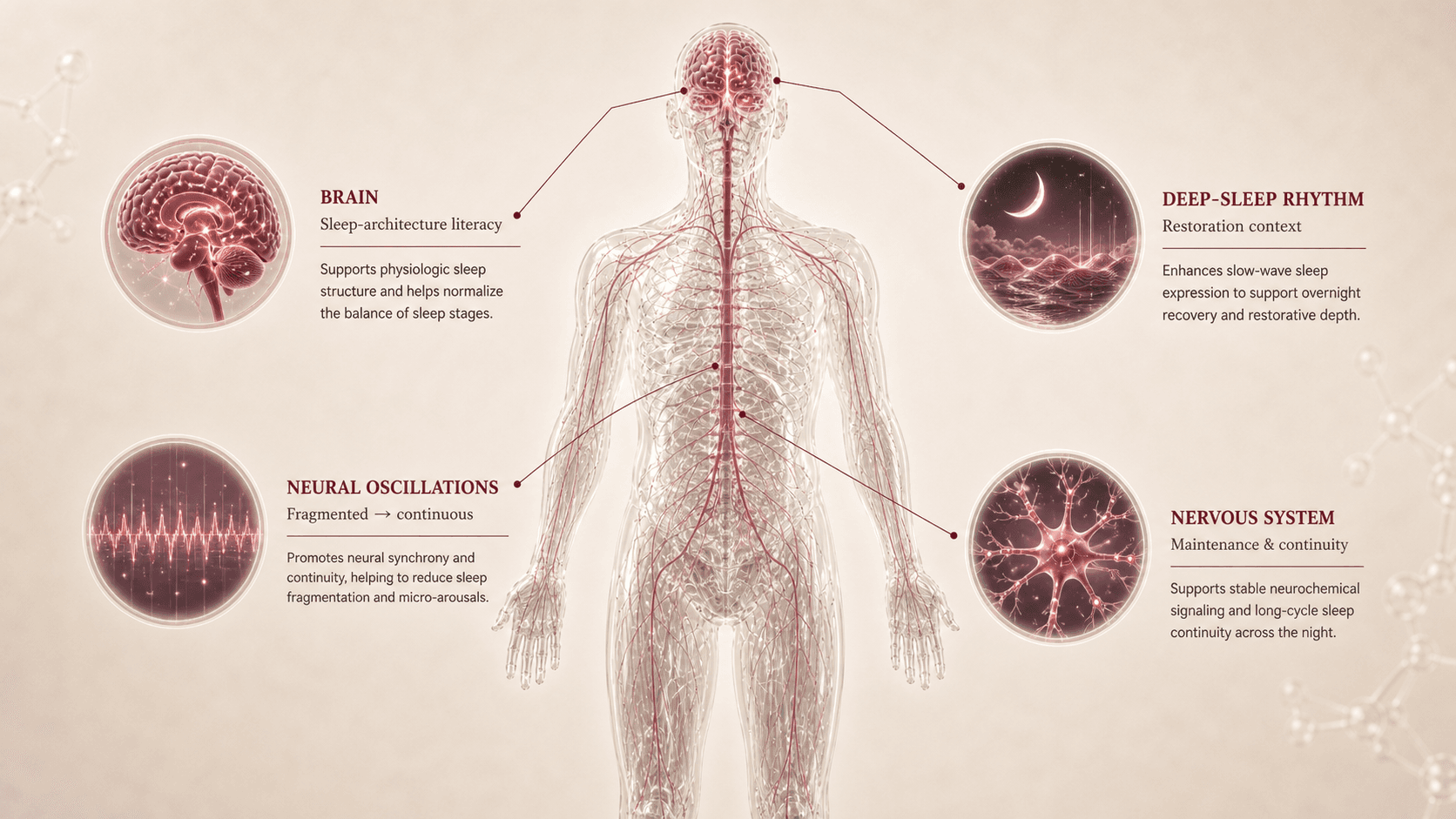 DSIP delta sleep-inducing peptide - emideltide | 78 | xDresearch only | subcutaneous - no protocol timeline | View |
| 03 | 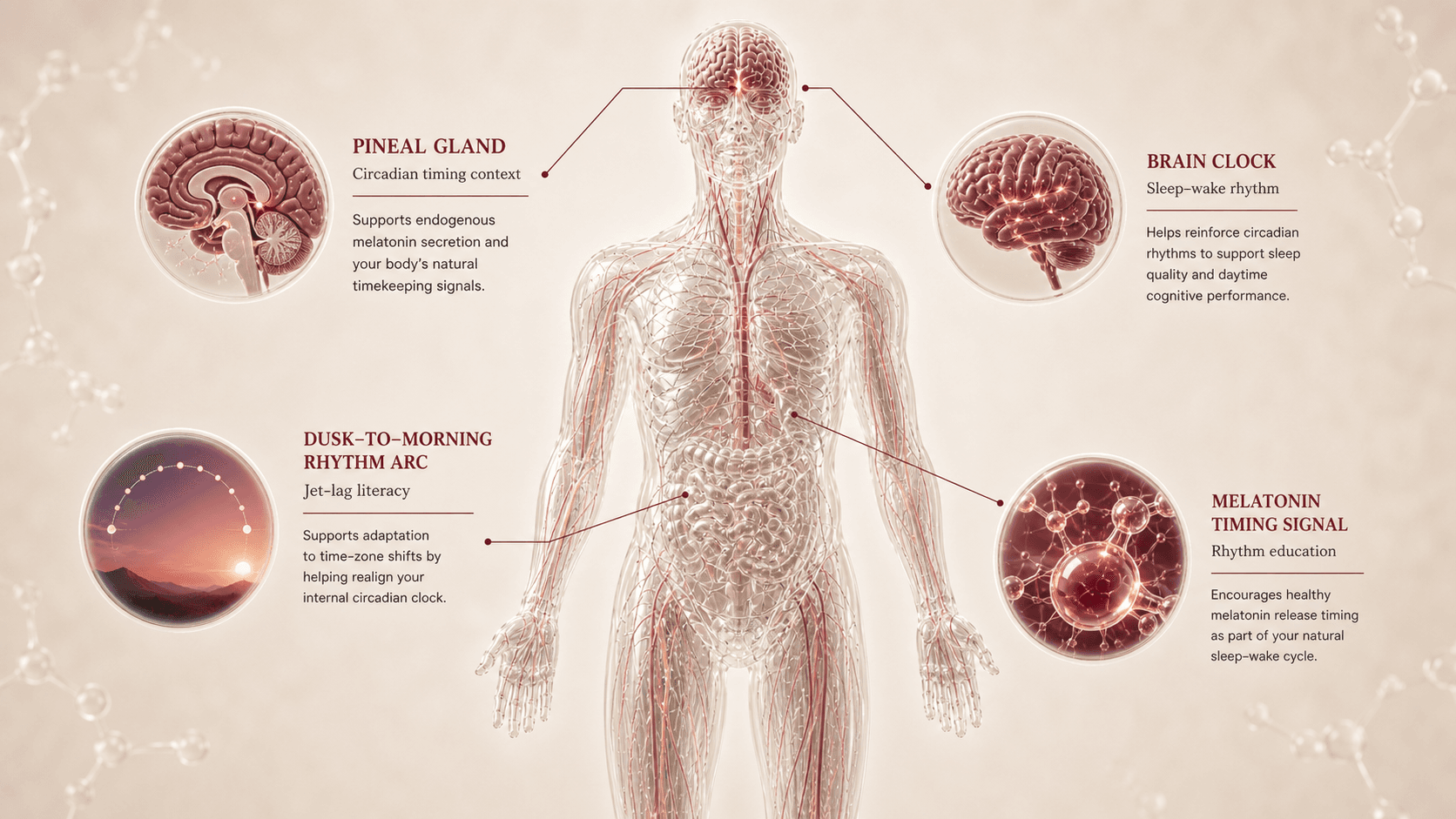 Epitalon / Epithalon epithalon - epitalon tetrapeptide | 74 | xCresearch only | subcutaneous - no protocol timeline | View |
| 04 | 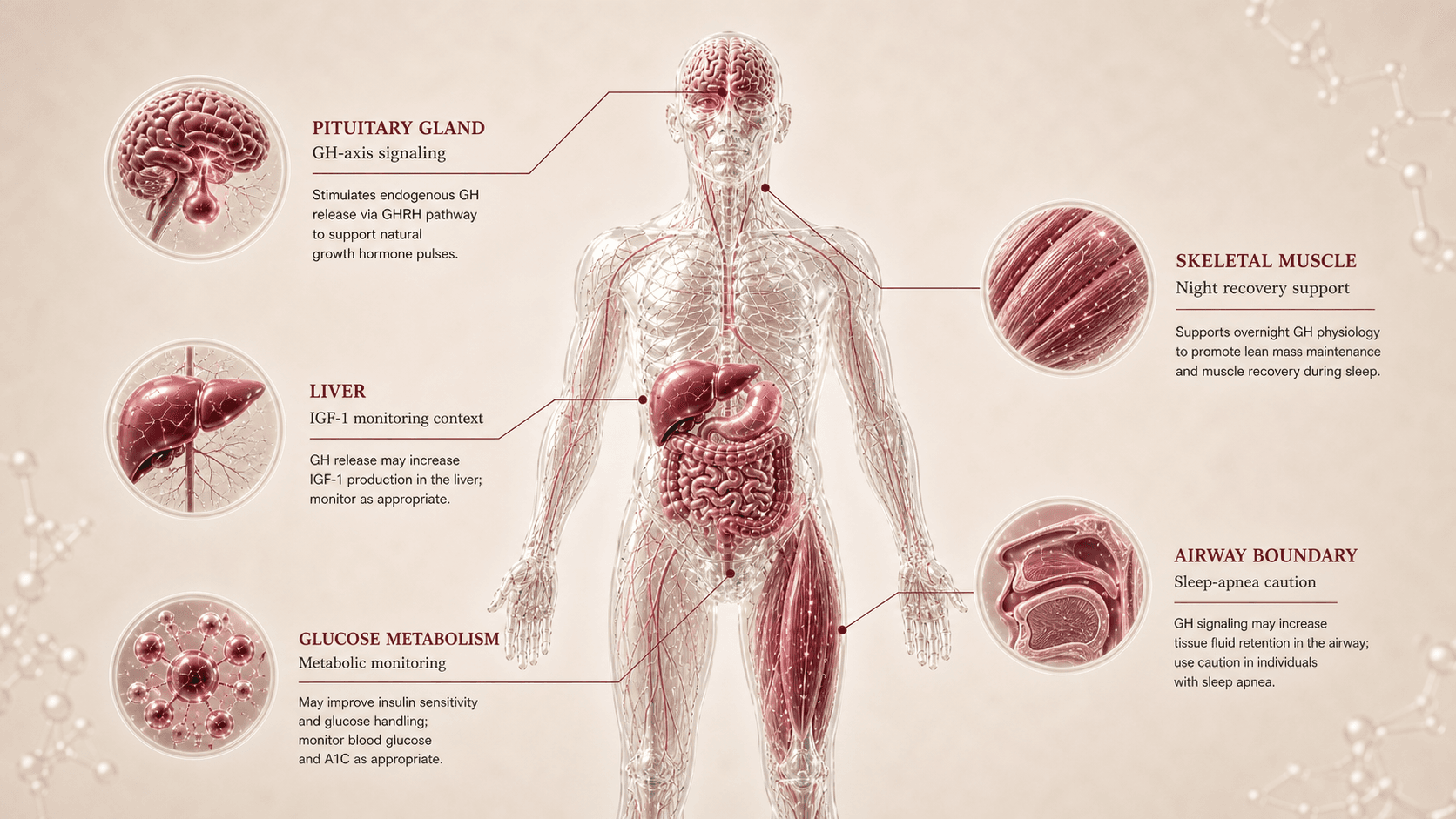 Ipamorelin ipamorelin acetate | 68 | xCresearch only | subcutaneous - no protocol timeline | View |
| 05 | 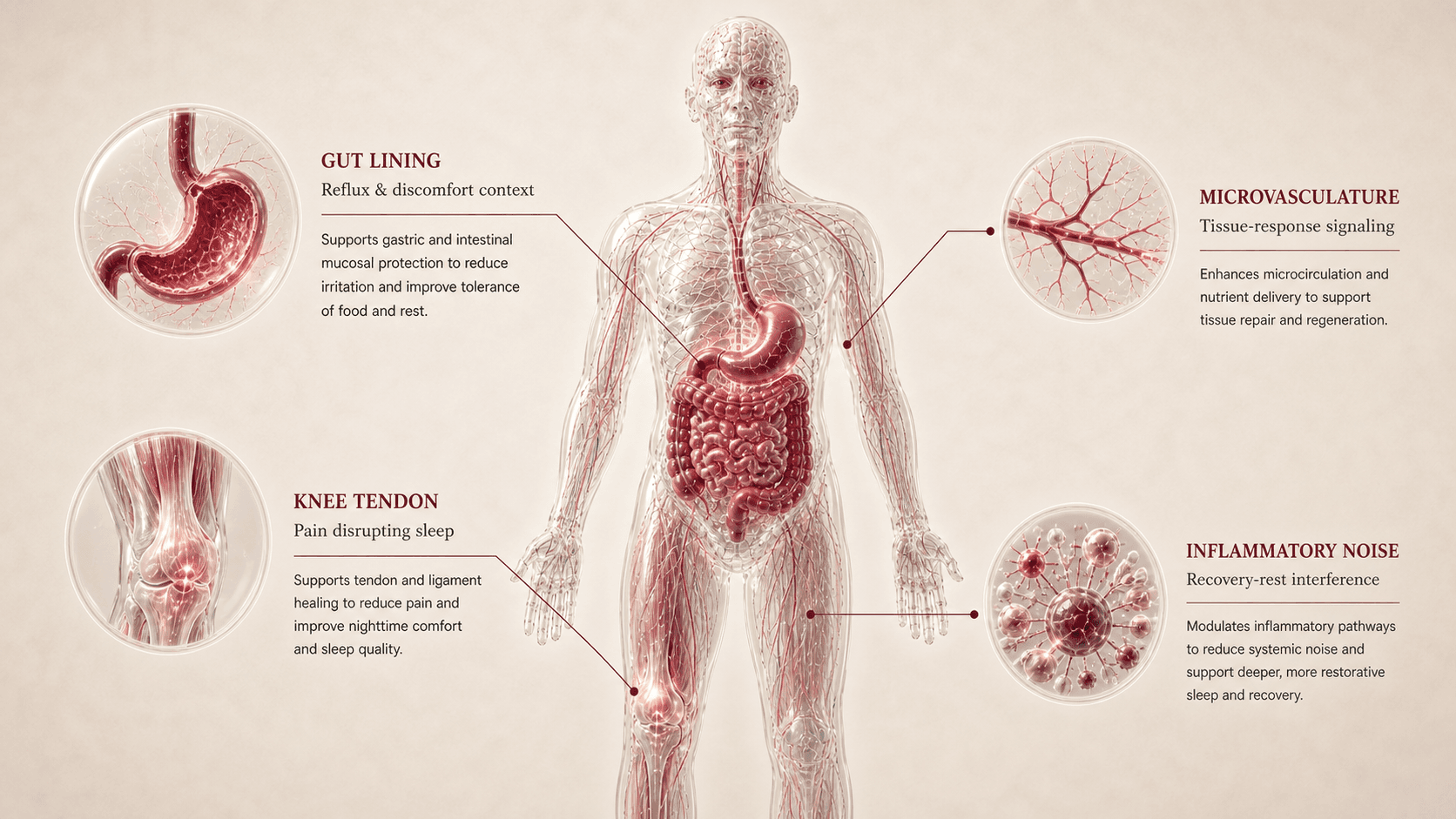 BPC-157 body protection compound 157 - bepecin | 62 | ~B-research only | subcutaneous - no protocol timeline | View |
Sleep & Rest comparison matrix
| Peptide | Regulatory anchor | Mechanism | Sleep pattern fit | Evidence maturity | Readiness | Watchout | Takeaway |
|---|---|---|---|---|---|---|---|
Selank selank | FDA safety-risk compounding page for Selank acetate plus stress/neuropeptide literature. | Neuropeptide / anxiolytic-nootropic / HPA-axis and neuroimmune context. | Sleep onset, anxious mind, stress-arousal, and HPA-axis load. Stress-arousal peptide for nights when the mind will not downshift. | Mechanistic and regional human interest; direct sleep-outcome evidence is limited and indirect. | Low/moderate; useful for education, not as an insomnia treatment or sleeping pill. | Not a sedative, not a hypnotic, and not a replacement for CBT-I, mental-health care, or medication review. | Best conceptual fit when sleep fails because stress and arousal stay high. |
DSIP dsip | FDA safety-risk compounding page for Emideltide (DSIP) plus sleep-architecture literature. | Sleep-regulation peptide / architecture and continuity claims. | Sleep maintenance, fragmentation, and sleep-architecture literacy. Classic sleep-architecture peptide with high market interest and high uncertainty. | Mixed and contradictory sleep literature; stronger as market-literacy content than as a proven outcome tool. | Low; no approved sleep label and no reliable consumer protocol should be inferred. | High uncertainty and overclaiming risk around deep sleep, REM, and sleep maintenance. | Included because users search for it, but the evidence caution is central. |
Epitalon / Epithalon epitalon | FDA safety-risk compounding page for Epitalon plus pineal/circadian literature. | Pineal / circadian / melatonin-rhythm and aging-biology claims. | Circadian rhythm, jet lag, timing drift, and pineal/melatonin literacy. Circadian-context peptide for timing and rhythm education. | Mechanistic and regional anti-aging/circadian interest; direct sleep-rest outcomes remain limited. | Low; useful for circadian literacy, not as a clinical rhythm-reset promise. | High overclaiming risk around anti-aging, pineal reset, telomeres, and guaranteed circadian regulation. | Relevant when the sleep problem looks like timing, rhythm, or jet-lag disruption. |
Ipamorelin ipamorelin | FDA safety-risk compounding page for ipamorelin acetate plus GH secretagogue literature. | GHSR agonist / GH secretagogue / recovery and IGF-1 context. | Non-restorative sleep, recovery sleep, GH-axis, and training-recovery overlap. GH-axis peptide for recovery-sleep literacy when enough sleep still does not feel restorative. | Selective GH-secretagogue biology with indirect sleep/recovery evidence and limited direct sleep outcomes. | Low/moderate; requires apnea, glucose, IGF-1, edema, endocrine, and cancer-history review. | Suspected apnea and GH-axis monitoring lower practical fit for Ana. | Relevant to recovery sleep, but not a sleep medication. |
BPC-157 bpc-157 | FDA safety-risk compounding page for BPC-157 plus existing Recovery and Gut Health source context. | Tissue-repair / gut-barrier / inflammatory-modulation hypotheses. | Pain, gut discomfort, reflux, recovery, and inflammation overlap that can disrupt sleep. Recovery-overlap peptide when discomfort is the reason sleep breaks. | Mechanistic and preclinical-heavy recovery/gut interest; sleep relevance is indirect. | Low/moderate; diagnosis, rehab, reflux/gut review, and source quality come first. | Not a sleep peptide; do not use pain or reflux as a reason to bypass diagnosis. | Relevant only when pain, gut, or recovery friction is fragmenting rest. |
CJC-1295 cjc-1295 | GH-axis comparator with FDA safety-risk compounding caution; no sleep label. | GHRH analog / GH-IGF-1 axis. | Adjacent GH-axis recovery-sleep comparator, especially when users discuss pairing with Ipamorelin. | Mechanistic GH-axis evidence; indirect and limited human sleep/rest outcome evidence. | Low/moderate; endocrine, IGF-1, glucose, edema, sleep-apnea, and cancer-history review. | Not a core sleep peptide and not a combination recommendation. | Useful for GH-axis literacy, not as a lead Sleep & Rest candidate. |
Melatonin melatonin | Non-peptide circadian context; US supplement regulation differs from drug approval and jurisdiction varies. | Circadian timing signal / melatonin receptor context. | Timing and jet-lag education, strongest for circadian timing rather than universal insomnia. | Context-specific evidence; not enough strong evidence to treat chronic insomnia broadly as solved by melatonin. | Variable by formulation, age, jurisdiction, and medication context. | Not a peptide and not a universal sleep fix. | Included because users know it first; read it as timing literacy. |
MK-677 / Ibutamoren mk-677 | Non-peptide GH secretagogue comparator; not a broad approved sleep therapy. | Ghrelin receptor agonist / GH secretagogue. | Deep-sleep and GH community comparator, not a Peptivius sleep peptide. | Limited sleep/rest outcome context with endocrine and metabolic caution. | Low for this niche; appetite, glucose, edema, endocrine effects, and bodybuilding drift matter. | Non-peptide, appetite/glucose/edema risk, and performance-market overclaiming. | Useful as a cautionary comparator when GH-secretagogue sleep claims appear online. |
MOTS-c mots-c | Adjacent mitochondrial/metabolic comparator; no sleep label. | Mitochondrial-derived peptide / AMPK / metabolic stress signaling. | Daytime fatigue and mitochondrial-resilience comparator when poor sleep becomes low energy. | Mechanistic mitochondrial plausibility; early and indirect for sleep/rest outcomes. | Low/moderate; belongs mainly to Longevity and Performance. | Should not be made a sleep peptide when insomnia, apnea, or circadian timing is the issue. | Useful only when daytime fatigue and metabolic resilience dominate the story. |
Sleep & Rest Combination & Overlap Map
| Combination | Components | Type | Why it appears | Peptivius read | Main caution | Status |
|---|---|---|---|---|---|---|
Selank + CBT-I / stress reduction / sleep routine | Selank + behavioral sleep foundation | Stress-arousal support context | Users with racing thoughts often search for calming compounds. | Educational stress-arousal context, not a replacement for CBT-I or mental-health care. | Do not treat Selank as a sleeping pill or psychiatric medication substitute. | Support foundation |
DSIP + sleep maintenance claims | DSIP + architecture/maintenance narrative | Sleep-architecture claim | DSIP has a classic sleep-peptide reputation and strong market interest. | Useful to explain the market narrative, but evidence remains mixed. | No deep-sleep guarantee and no approved sleep label. | High uncertainty |
Epitalon + melatonin / circadian context | Epitalon + melatonin timing education | Circadian rhythm overlap | Both are discussed around pineal, timing, jet lag, and rhythm. | Circadian literacy only, not a universal insomnia fix. | Melatonin is non-peptide; Epitalon has limited evidence and no sleep label. | Adjacent education |
Ipamorelin + CJC-1295 | GH-axis secretagogue pairing | GH-axis recovery-sleep overlap | The pairing is common in GH-axis and recovery communities. | Compatibility education, not a combination instruction. | IGF-1, glucose, edema, sleep apnea, endocrine context, and cancer-history review. | Professional review / not casual |
BPC-157 + pain/gut disrupting sleep | BPC-157 + pain, reflux, gut, and recovery foundation | Recovery/gut overlap | Pain, reflux, gut discomfort, and inflammation can fragment sleep. | Useful when discomfort is the sleep driver, not as a sleep peptide. | Diagnose pain, reflux, or gut symptoms first. | Overlap context |
Z-drugs / benzodiazepines | Medication context, not a peptide combination plan | Medication boundary | Users often compare being sedated with getting restorative sleep. | Sleep-inducing medication is not the same as restorative sleep architecture. | Chronic use requires professional review and medication-context interpretation. | Medical review boundary |
Melatonin + Epitalon | Non-peptide timing signal + pineal-context peptide | Non-peptide circadian context | Both appear in circadian and jet-lag discussions. | Timing/rhythm education only. | Do not convert into a circadian combination recommendation. | Do not treat as a plan |
Frequent questions about Sleep & Rest peptides
Is Sleep & Rest for insomnia?
It is a sleep-pattern education module, not an insomnia treatment. Chronic insomnia should bring CBT-I and clinical evaluation into the foreground.
Can peptides replace CBT-I?
No. CBT-I remains a foundation for chronic insomnia context. Peptides in this report are not behavioral therapy replacements.
Does DSIP really work?
DSIP is included because of sleep-architecture history and market interest, but the evidence is mixed and should be read cautiously.
Is Selank a sleeping pill?
No. Selank is framed as stress-arousal literacy, not sedation or an insomnia medication.
Does Epitalon regulate melatonin?
Epitalon appears in pineal and circadian discussions, but Peptivius does not claim guaranteed clinical melatonin regulation or rhythm reset.
Can Ipamorelin improve deep sleep?
Ipamorelin is a GH-axis recovery-sleep topic, not a direct sleep medication. Any deep-sleep claim should be read as indirect and cautious.
What if my real problem is sleep apnea?
Then apnea evaluation comes first. Suspected apnea is especially important before interpreting GH-axis compounds.
What changes if I use Zolpidem, Clonazepam, or other sleep medications?
Medication context becomes central. The report can explain architecture vs sedation, but medication review belongs with a licensed professional.
Why is Melatonin included if it is not a peptide?
Because users know it first. It belongs as non-peptide circadian timing context, not as a peptide candidate.
Why is BPC-157 in Sleep & Rest?
Only because pain, gut discomfort, reflux, and recovery problems can interrupt sleep. It is not a sleep peptide.
Can peptides fix sleep if caffeine, alcohol, or stress are the issue?
No peptide should be used to avoid obvious sleep foundations. Caffeine timing, alcohol, stress, light, routine, and recovery load can dominate the outcome.
Does Peptivius create a sleep combination plan?
No. The Combination & Overlap Map explains narratives users encounter. It does not recommend combinations or operational protocols.
Final personalized interpretation for Ana Beatriz
Ana's Sleep & Rest pattern is mixed: about 5.5 hours of sleep, subjective quality 2/5, difficulty falling asleep and staying asleep, high stress, anxiety treated with an SSRI, next-day brain fog, occasional jet lag, suspected apnea, and recovery/gut context. That is why the section starts with foundation rather than a peptide list.
Selank ranks first because the strongest visible pattern is stress-arousal: the mind does not downshift cleanly at night. DSIP remains relevant because maintenance and architecture are part of the story, but its evidence caution is unusually important. Epitalon enters through circadian timing and travel disruption, not as a guaranteed rhythm reset.
Ipamorelin is relevant only as recovery-sleep and GH-axis literacy. It should be read carefully because suspected apnea, PCOS/metabolic context, glucose monitoring, IGF-1, edema, and endocrine review reduce practical fit. BPC-157 belongs only if pain, gut discomfort, reflux, or recovery friction is fragmenting sleep.
CJC-1295 is a GH-axis comparator rather than a core Sleep & Rest peptide. Melatonin is included only as non-peptide circadian context. MK-677 and MOTS-c belong in adjacent comparison, not as peptide ranking leads.
For Ana, the most important Sleep & Rest intervention is still the foundation: regular timing, morning light, evening light boundaries, caffeine timing, apnea evaluation, stress and CBT-I context, pain/reflux review, medication review, and recovery planning. Peptides are educational mechanism discussions after those questions are visible.