Hormonal Health.
7 peptides, ranked.
Hormonal Health is the Blueprint layer for PCOS, Hashimoto, cycle irregularity, reproductive-axis signaling, GH/IGF-1 overlap, metabolic hormones, fatigue, and medication/lab interpretation. Each candidate was evaluated against your BioProfile, training load, and declared contraindications. The strongest matches sit at the top; secondary options remain visible for comparison.
Hormonal foundation - before peptides
Hormonal Health starts with diagnosis, labs, medication context, cycle history, thyroid stability, PCOS phenotype, sleep, nutrition, and metabolic markers before peptide mechanisms are interpretable.
- Thyroid status, levothyroxine timing/adherence, TSH/free T4/free T3 context, antibodies when relevant, and symptom pattern.
- PCOS phenotype: cycle pattern, acne/hirsutism, SHBG, testosterone/free androgen index, insulin resistance, and metformin context.
- Fertility intent, pregnancy possibility, lactation, contraception, and gynecologic review.
- Glucose, HbA1c, fasting insulin, lipids, liver markers, body-composition trend, sleep apnea, stress, and calorie availability.
- Medication review before interpreting reproductive, thyroid, GH-axis, or sexual-function symptoms.
Hormonal red flags - when this is not a peptide question
Endocrine symptoms can reflect medical disease, medication effects, pregnancy/fertility context, or urgent findings. These boundaries come before peptide ranking.
- Pregnancy, active fertility treatment, amenorrhea, abnormal bleeding, severe pelvic pain, galactorrhea, or rapid virilization.
- Uncontrolled thyroid disease, adrenal symptoms, pituitary symptoms, severe hypoglycemia, or unexplained rapid weight change.
- Severe depression, eating-disorder risk, overtraining, under-fueling, or suspected sleep apnea.
- Cancer history, active malignancy, severe cardiovascular risk, or endocrine tumor concern.
- Any hormone-active medication changes without clinician review.
Ranked list
| Rank | Peptide | Match | Evidence | Regimen | |
|---|---|---|---|---|---|
| 01 | 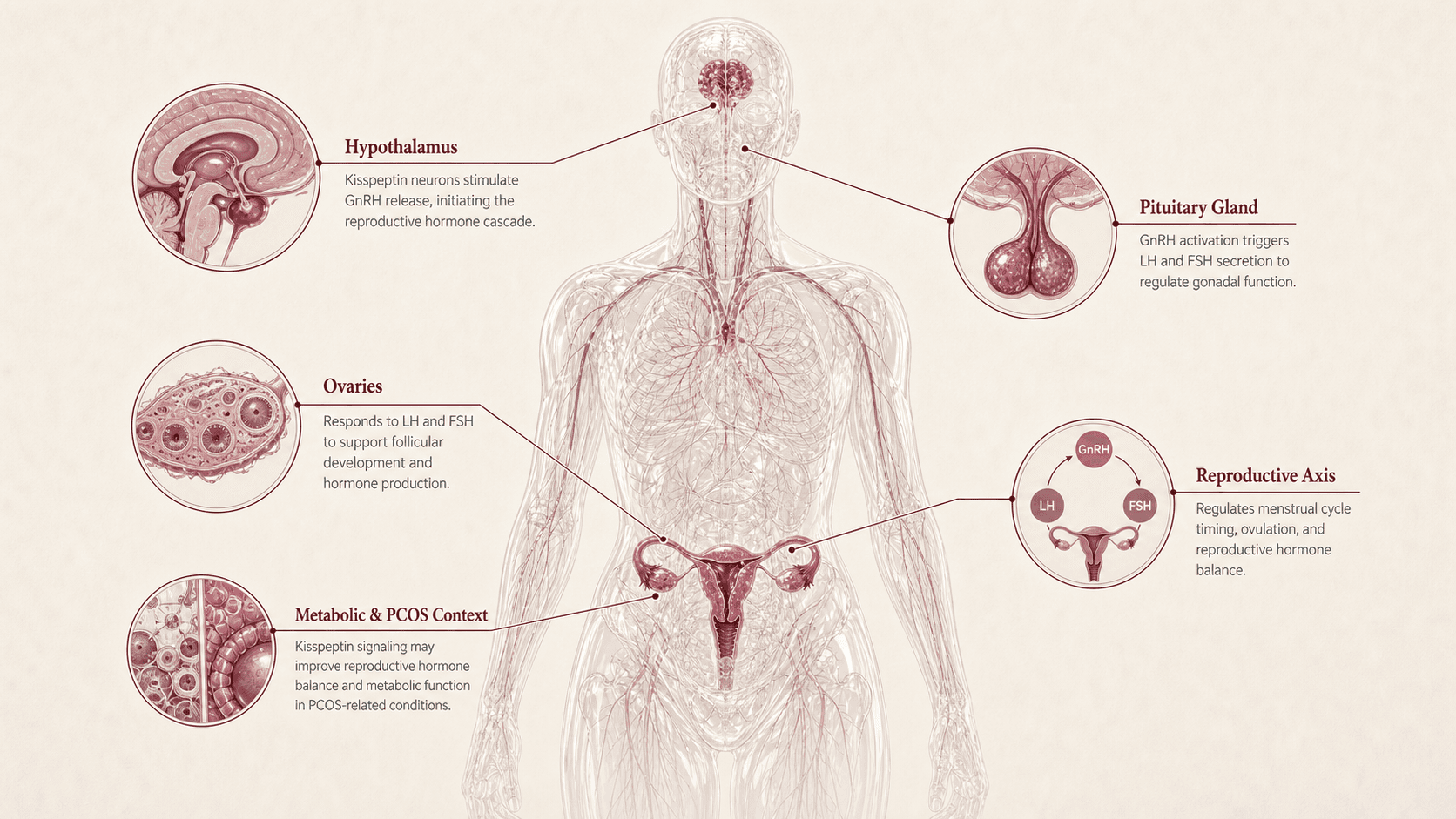 Kisspeptin kisspeptin-54 - kisspeptin-10 | 84 | ~B-phase 2 | subcutaneous - no protocol timeline | View |
| 02 | 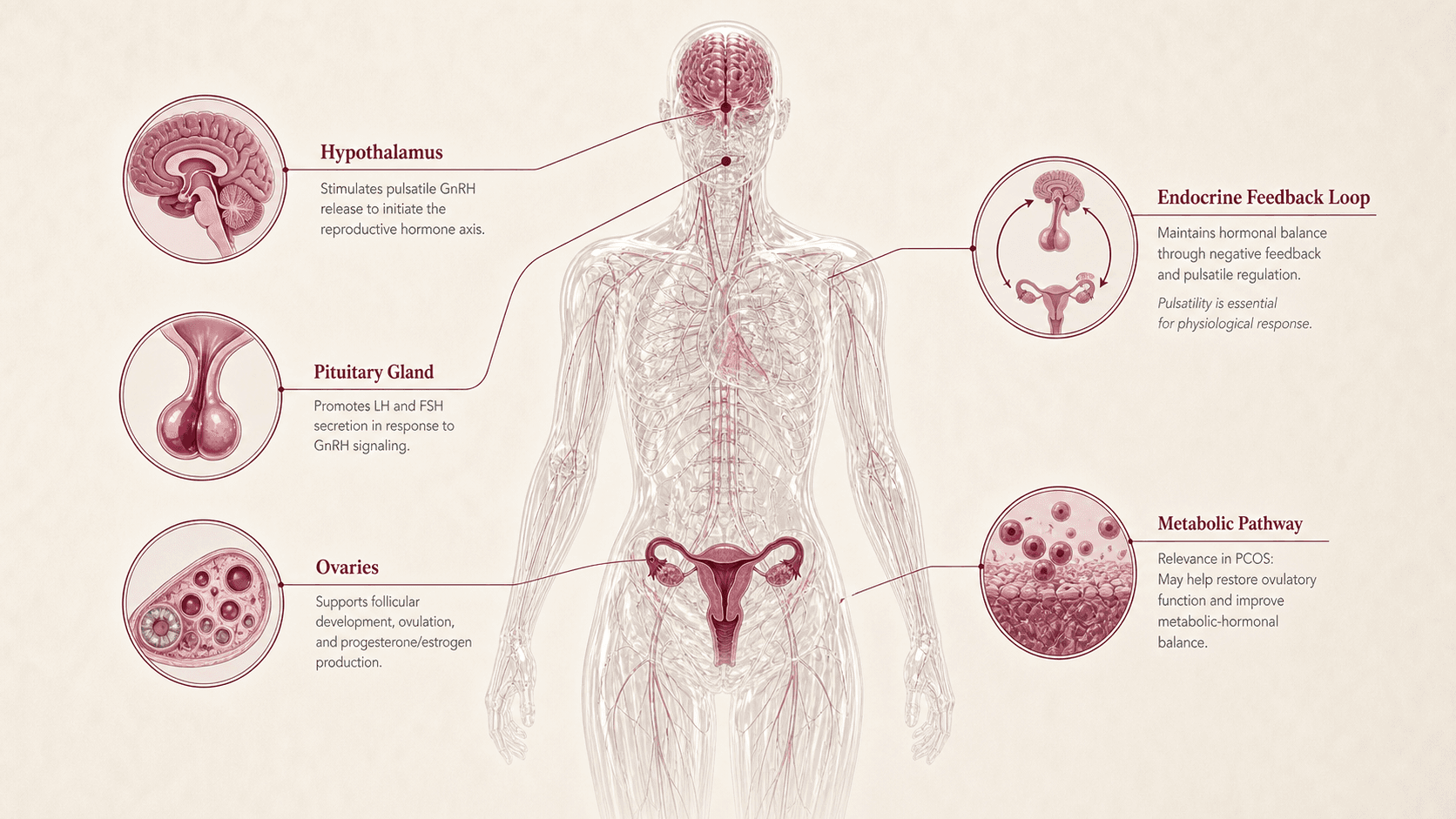 Gonadorelin gnrh - lhrh | 80 | ~Bfda approved | subcutaneous - no protocol timeline | View |
| 03 | 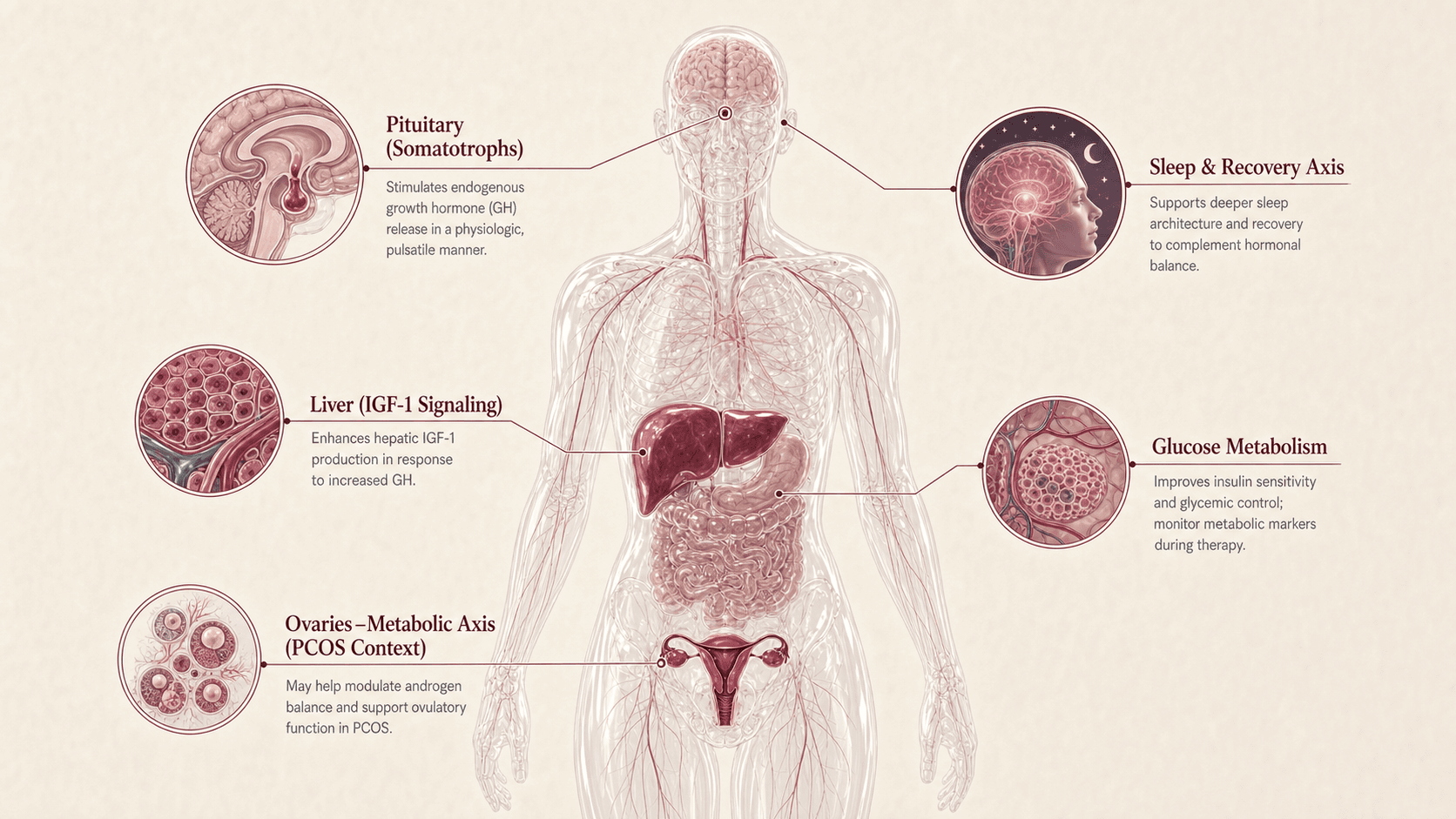 Sermorelin ghrh 1-29 - grf 1-29 | 74 | xCresearch only | subcutaneous - no protocol timeline | View |
| 04 | 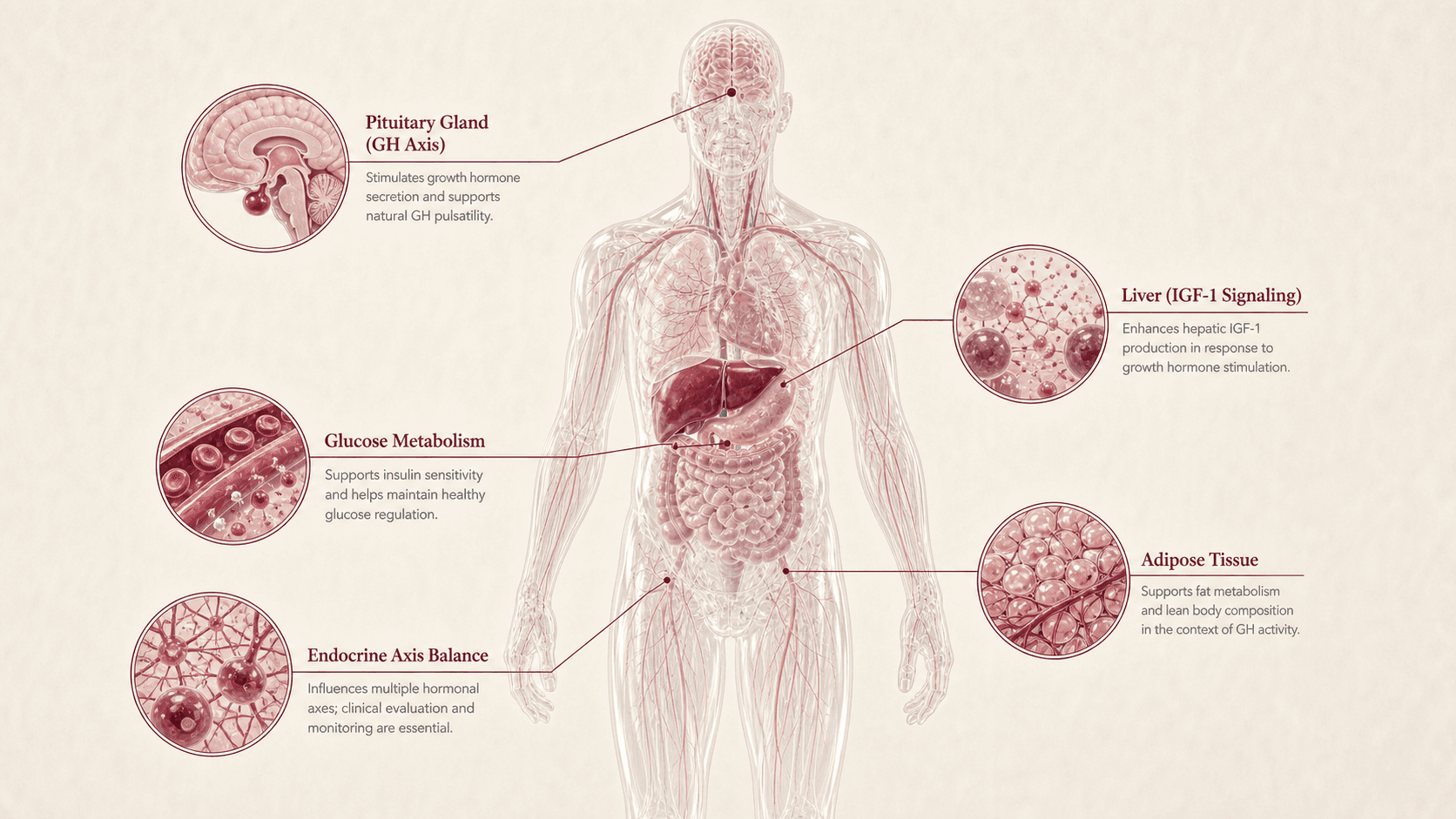 CJC-1295 modified grf - cjc-1295 dac | 70 | xCresearch only | subcutaneous - no protocol timeline | View |
| 05 | 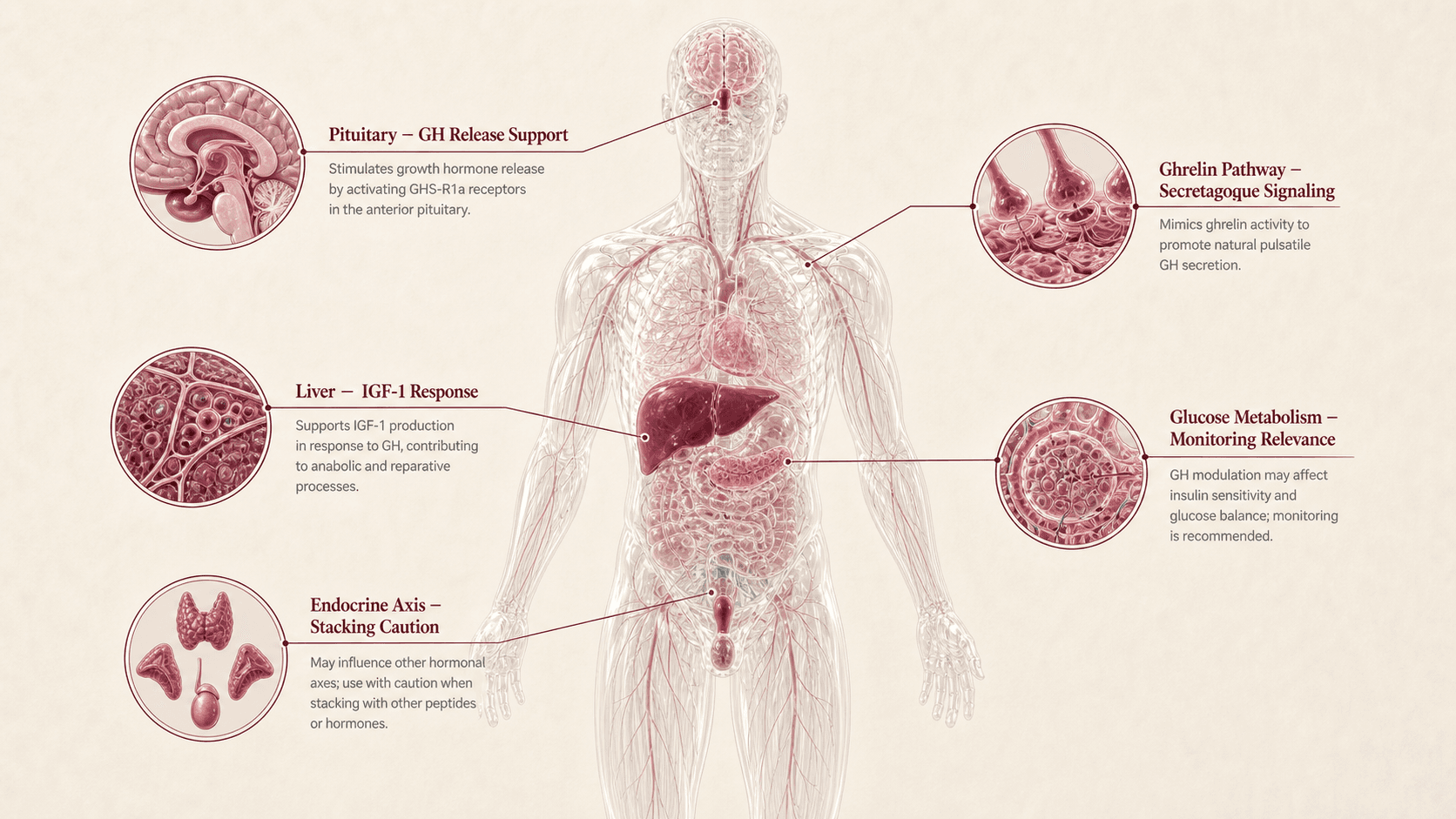 Ipamorelin ipamorelin acetate | 68 | xCresearch only | subcutaneous - no protocol timeline | View |
| 06 | 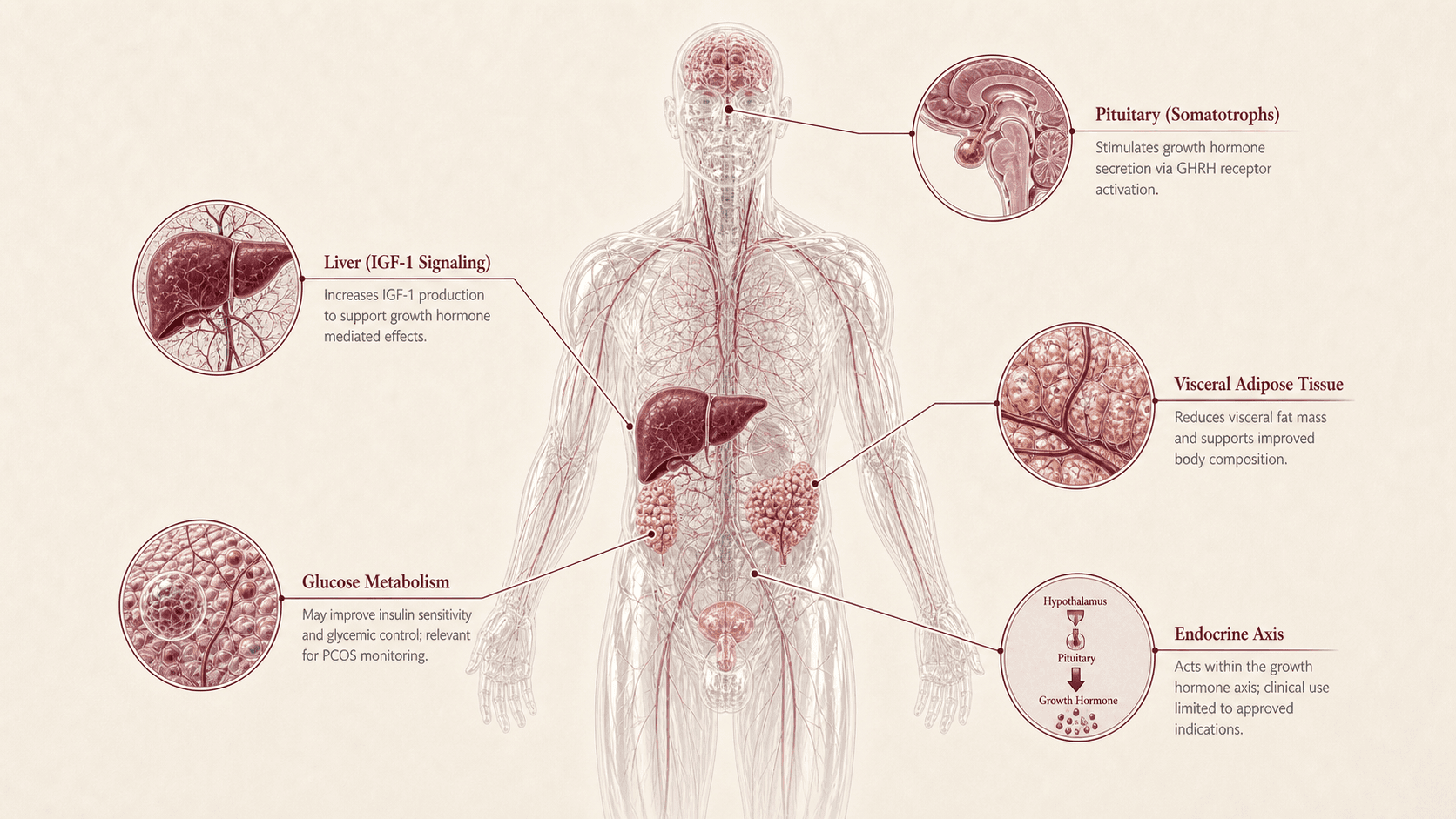 Tesamorelin egrifta wr - egrifta sv | 66 | ~Bfda approved | subcutaneous - no protocol timeline | View |
| 07 | 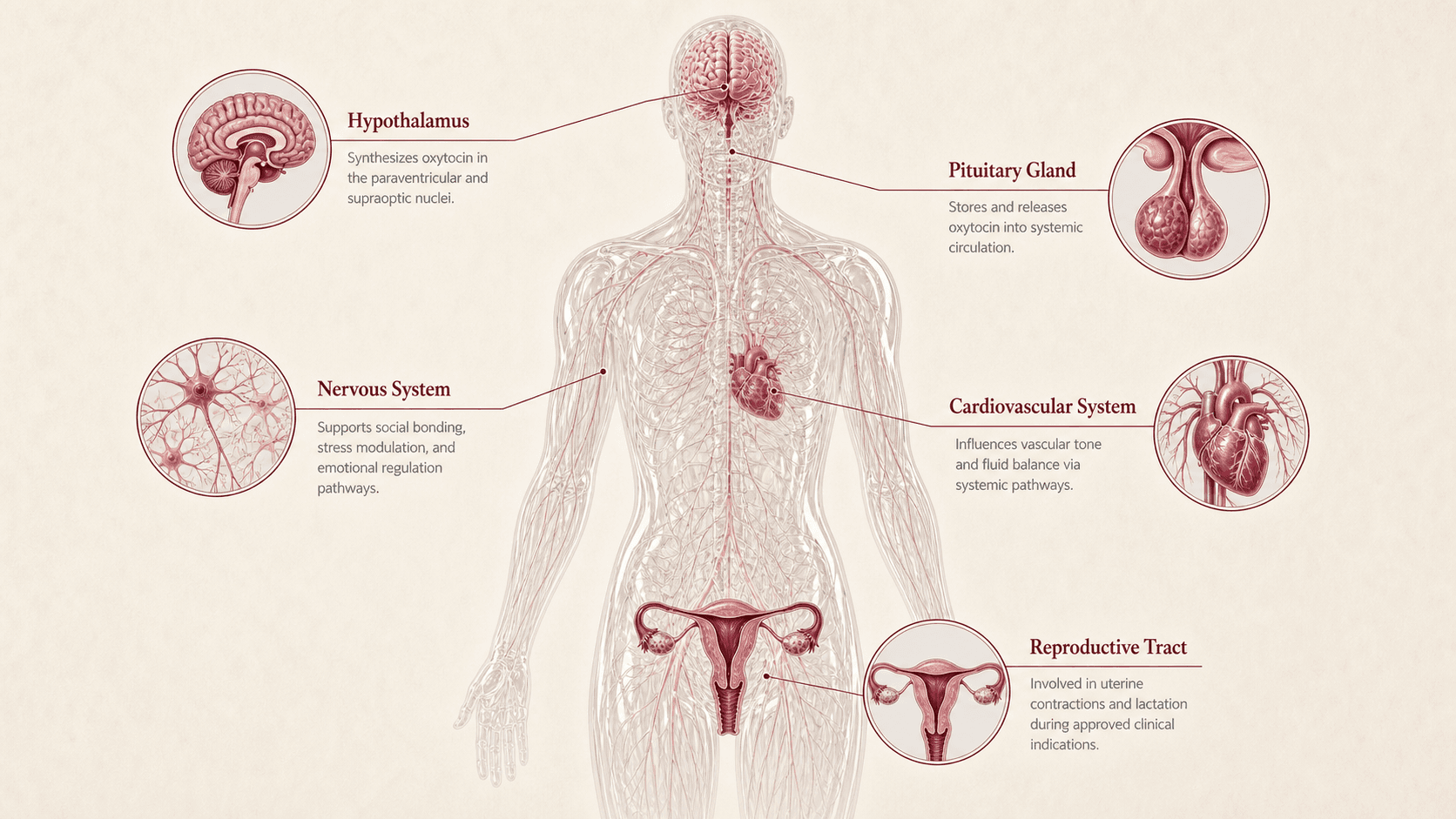 Oxytocin oxt | 58 | xCfda approved | intranasal - no protocol timeline | View |
Hormonal Health comparison matrix
| Peptide | Regulatory anchor | Mechanism | Hormonal role | Evidence maturity | Readiness | Watchout | Takeaway |
|---|---|---|---|---|---|---|---|
Kisspeptin kisspeptin | PubMed/JCI kisspeptin receptor agonist and reproductive endocrine literature. | Kisspeptin-GnRH / reproductive-axis signaling. | Reproductive-axis and gonadotropin signaling literacy. | Human mechanistic and reproductive-endocrine studies exist; broad consumer hormonal use is not established. | Low outside specialist reproductive/endocrine contexts. | Fertility, cycle, pregnancy, pituitary, and PCOS context require clinical review. | Best reproductive-axis anchor, but not a self-directed hormone tool. |
Gonadorelin gonadorelin | Gonadorelin label/diagnostic and reproductive-axis clinical context. | GnRH / LH-FSH axis. | Pituitary-gonadal axis and diagnostic/fertility-context literacy. | Known endocrine pharmacology and historical label contexts; consumer hormone-clinic use needs caution. | Medium only in proper clinical context; low for wellness extrapolation. | Pulsatility, indication, fertility, pituitary, and hormone-monitoring context are central. | A real endocrine anchor, not a casual hormone optimizer. |
Sermorelin sermorelin-hormonal | Existing Sermorelin GH-axis dossier and clinical context. | GHRH / GH-IGF-1 axis. | GH-axis literacy for fatigue, sleep, body composition, and endocrine monitoring. | Known GH-axis biology; limited direct evidence for Ana's hormonal concerns. | Low/moderate; IGF-1, glucose, edema, sleep apnea, and cancer-history review. | GH-axis signaling can complicate PCOS/metabolic and sleep-apnea context. | Useful GH-axis comparator, secondary to PCOS and thyroid foundations. |
CJC-1295 cjc-1295-hormonal | FDA safety-risk compounding page for CJC-1295 plus GH-axis context. | GHRH analog / GH-IGF-1 axis. | Stronger GH-axis signaling and anti-aging clinic literacy. | Mechanistic GH/IGF-1 evidence; limited wellness outcomes and FDA safety-risk concerns. | Low; monitoring burden is high. | IGF-1, glucose, edema, sleep apnea, cancer/endocrine history, and GH-axis stacking. | Important to understand, but not a casual endocrine option. |
Ipamorelin ipamorelin-hormonal | FDA safety-risk compounding page for ipamorelin acetate plus GH secretagogue context. | GHSR agonist / GH secretagogue. | GH secretagogue and CJC pairing literacy. | Selective secretagogue biology; limited direct endocrine-wellness outcomes. | Low; route safety and GH-axis monitoring matter. | Often paired with CJC-1295, reducing attribution and increasing monitoring burden. | Relevant to explain, but not a primary Hormonal Health match. |
Tesamorelin tesamorelin-hormonal | Egrifta label context for excess abdominal fat in HIV-associated lipodystrophy. | GHRH analog / GH-IGF-1 / visceral-fat context. | Adjacent body-composition and metabolic hormone comparator. | Strongest in narrow HIV-lipodystrophy indication; limited for PCOS or broad hormone wellness. | Medium only in label-aligned care; low as general Hormonal Health. | Indication mismatch, glucose/IGF-1 monitoring, edema, and malignancy/endocrine review. | Legitimate but narrow; not a PCOS or thyroid peptide. |
Oxytocin oxytocin-hormonal | Oxytocin approved-drug and neuroendocrine literature. | Neuropeptide hormone / social, reproductive, and uterine context. | Hormone-peptide literacy and bridge to Sexual Wellness. | Strong in obstetric approved contexts; mixed and indication-specific for broader neuroendocrine claims. | Low for Hormonal Health outside approved/clinical context. | Approved obstetric context should not be generalized to mood, libido, or hormone wellness. | Useful as hormone-peptide context, not a PCOS or thyroid tool. |
Hormonal Health Combination & Overlap Map
| Combination | Components | Type | Why it appears | Peptivius read | Main caution | Status |
|---|---|---|---|---|---|---|
Kisspeptin + Gonadorelin | Kisspeptin pathway + GnRH/LH/FSH axis | Reproductive-axis overlap | Both sit upstream of gonadotropin signaling. | Useful for axis literacy, not a fertility or hormone protocol. | Cycle, fertility, pregnancy, pituitary, and PCOS context require clinical review. | Professional review |
CJC-1295 + Ipamorelin | GHRH analog + GH secretagogue | GH-axis pairing | Common in body-composition and anti-aging clinics. | Mechanism overlap with high monitoring burden. | IGF-1, glucose, edema, sleep apnea, cancer/endocrine history. | Not casual |
Tesamorelin + metabolic/PCOS context | GHRH analog + visceral-fat/metabolic discussion | Adjacent indication context | Visceral fat and insulin resistance overlap with PCOS conversations. | Narrow approved context should not be generalized. | Indication mismatch and glucose/IGF-1 monitoring. | Adjacent education |
Thyroid/PCOS care | Non-peptide endocrine foundation | Clinical foundation | Ana's strongest hormone signals are PCOS and Hashimoto. | Most important first layer. | Do not use peptide novelty to bypass endocrine care. | Support foundation |
Frequent questions about Hormonal Health peptides
Is this a hormone protocol?
No. It is endocrine literacy and ranking, not a protocol.
Why do Kisspeptin and Gonadorelin rank high?
They map directly to reproductive-axis signaling, but clinical context is decisive.
Are GH-axis peptides hormonal?
Yes. CJC-1295, Ipamorelin, Sermorelin, and Tesamorelin require GH/IGF-1 and metabolic safety framing.
Can peptides treat PCOS or Hashimoto?
This report does not claim that. PCOS and Hashimoto remain clinical care contexts.
Why include Oxytocin?
It is a hormone-peptide context users encounter, but it is not a PCOS or thyroid treatment.
Final personalized interpretation for Ana Beatriz
Ana's Hormonal Health module is anchored by PCOS, Hashimoto, levothyroxine, metformin, fatigue, cycle irregularity, body-composition concern, and poor sleep.
Kisspeptin and Gonadorelin lead because they explain the reproductive axis. Sermorelin, CJC-1295, Ipamorelin, and Tesamorelin explain GH/IGF-1 and body-composition overlap, but they carry heavier monitoring boundaries.
Oxytocin is included as a hormone-peptide context and bridge to Sexual Wellness, not as a thyroid, PCOS, or cycle treatment.
For Ana, endocrine clarity means thyroid stability, PCOS labs, glucose/insulin context, sleep-apnea screening, cycle/fertility review, and medication interpretation before peptide mechanisms.