BPC-157
The central recovery conversation peptide, strongest for localized tendon and ligament discussion but still research-sensitive.
Synthetic 15-amino-acid pentadecapeptide discussed in tissue-repair, vascular, gut, and musculoskeletal models.
BPC-157 is highly visible in injury-recovery communities because preclinical literature is broad and the anecdotal signal is loud. The Blueprint keeps the useful part and the boundary together: it can be relevant to chronic tendon or localized tissue-support questions, but it is not an approved human healing drug and should not replace diagnosis or rehab.
Why it may make sense for you
For Ana, BPC-157 rises to the top because the recovery problem is concrete: chronic left patellar tendinopathy limiting training. Data confidence is Medium: the match is readable, but it would be stronger with a detailed orthopedic diagnosis, recent imaging, a functional pain scale, and a more structured rehab history.
| Signal | Interpretation |
|---|---|
| Primary recovery signal | Chronic patellar tendinopathy with training limitation |
| Category fit | Localized tendon and connective-tissue discussion |
| Data confidence | Medium - clear chronic tendon signal, but diagnosis, imaging, functional scale, and rehab history remain incomplete. |
| Support context | Needs rehab/load management, not peptide-only logic |
| Main caution | Research-sensitive status and limited human translation |
- Best match for localized injury literacy.
- Does not require framing the problem as systemic fatigue.
- Can be evaluated against function, pain behavior, and rehab tolerance.
- Not a replacement for diagnosis, imaging, or progressive loading.
- Evidence maturity is lower than Weight Loss incretins.
- Quality and regulatory context matter heavily.
How it works
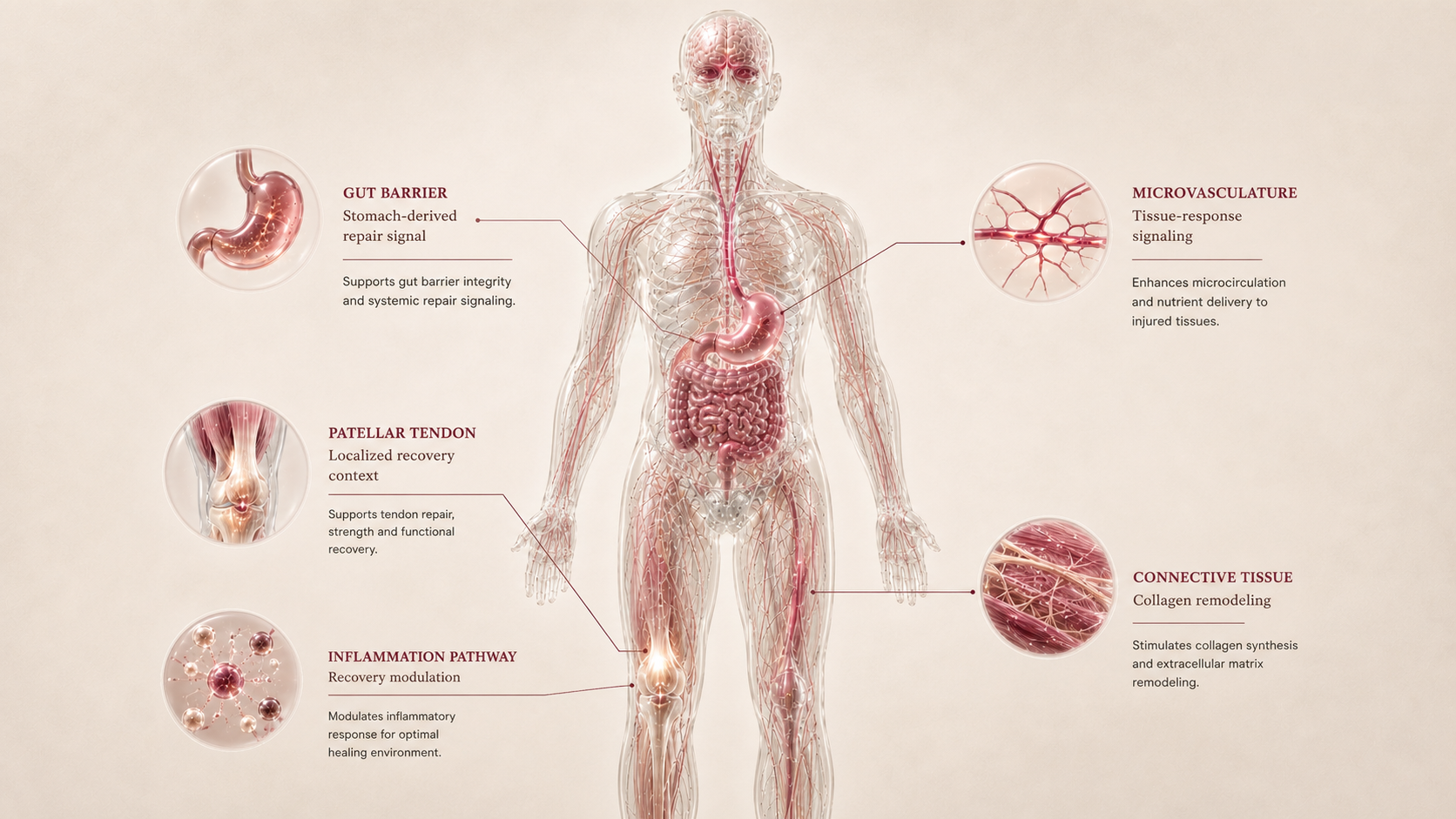
BPC-157 is discussed as a tissue-repair and cytoprotective peptide. The most relevant mechanisms for this niche are angiogenesis, fibroblast activity, local inflammation modulation, endothelial signaling, and tendon-cell migration hypotheses. These mechanisms are interesting, but they do not prove a universal human recovery protocol.
| Pathway | Practical effect |
|---|---|
| Tendon / ligament | Research models discuss fibroblast activity and remodeling signals. |
| Microvasculature | Angiogenesis and endothelial-signaling hypotheses appear in preclinical literature. |
| Inflammation | Local inflammatory modulation is discussed, but not as a diagnosis substitute. |
| Gut overlap | Gastric and barrier-protection research explains why gut-recovery claims appear. |
BPC-157 belongs in the recovery map because it points toward tissue-support biology, but the human decision still depends on diagnosis, rehab, and risk review.
What the evidence shows
BPC-157 has three evidence layers: mechanistic evidence is moderate/high in preclinical tissue-repair models; human outcome evidence for specific injuries remains low; regulatory/label evidence is absent for recovery because there is no approved human healing label.
| Study | Population | Key result | How to read it |
|---|---|---|---|
| Mechanistic evidence | Animal and cellular models | Signals around angiogenesis, fibroblast activity, cell outgrowth, survival, migration, and remodeling | Moderate/high preclinical signal, not a human protocol. |
| Human outcome evidence | Preclinical-heavy and limited human translation | Large controlled human tendon or ligament trials are lacking | Low for confirmed injury outcomes. |
| Regulatory / label evidence | FDA safety-risk / withdrawn nomination context | FDA flags immunogenicity, impurities, limited safety information, and API characterization concerns | No approved recovery label; regulatory caution belongs in the dossier. |
- Large, well-controlled human injury trials are lacking.
- Best human population, route, exposure pattern, and monitoring are not standardized here.
- Long-term safety and product-quality risk are not resolved by anecdotal popularity.
- Combination evidence is not the same as single-compound evidence.
Safety, side effects, and contraindications
- Injection-site or local irritation may be reported depending on product/route context.
- Unclear tolerability profile because human data are limited.
- Attribution problems when used inside blends.
- FDA safety-risk concerns for compounded BPC-157.
- Quality, purity, sterility, and identity uncertainty.
- Post-surgical, infection, severe injury, or worsening pain contexts require medical review.
- Possible concern around proliferative/angiogenic logic in active cancer or relevant oncology history.
- Active malignancy or unresolved oncology history without clinician review.
- Active infection or wound complication.
- Pregnancy or lactation without professional review.
- Unexplained severe pain, neurologic symptoms, acute rupture, or suspected fracture.
- Competitive sport context without anti-doping review.
- Acute trauma with intense pain, inability to bear weight, visible deformity, fever, heat, redness, discharge, progressive night pain, post-operative worsening, new bone pain with cancer history, or unexplained pain worsening despite rest.
For Ana, the main risk is treating knee tendinopathy as a peptide problem instead of a load, rehab, and diagnosis problem with a peptide discussion around it.
Reference protocol
Variable clinical context: BPC-157 is anchored to research-sensitive musculoskeletal literature and FDA safety-risk compounding framing, not to an approved human healing label.
- BPC-157 plus TB-500 blends
- KLOW-like multi-peptide recovery blends
- Community injury protocols
- Research-only vials treated as approved medication
- Vial, syringe, concentration, or unit conversion charts
| Item | Reference |
|---|---|
| Reference | Preclinical and limited human translation; no approved tendon, ligament, pain, or recovery label. |
| Route/frequency | Not standardized in an official label; this report does not provide a route schedule or application count. |
| Application footprint | Depends on diagnosis, injury depth, rehab plan, clinical oversight, and product quality. |
| Decision frame | Function, pain behavior, loading tolerance, imaging/procedure history, and adverse effects matter more than forum timelines. |
- Clarify whether the problem is tendon, ligament, muscle, joint, gut overlap, post-procedure healing, or nonspecific pain.
- A chronic tendinopathy is not read the same way as an acute tear, surgical wound, or inflammatory flare.
- The compound is interpreted alongside load management, progressive rehab, sleep, and protein adequacy.
- A peptide signal cannot compensate for continued overload of the injured tissue.
- Track function and training tolerance before assigning benefit to BPC-157.
- Avoid judging response when several recovery compounds or blends start together.
- Persistent pain, swelling, neurologic symptoms, post-surgical complications, or worsening function need professional reassessment.
- Stopping is a context review, not a universal taper.
| Item | Reference |
|---|---|
| Source anchor | Research-sensitive musculoskeletal literature plus FDA safety-risk compounding context. |
| Protocol status | No universal label, no application count, and no community protocol adopted. |
| Main dependency | Diagnosis, rehab, loading, product identity, and professional review. |
| Blend boundary | BPC-157 plus TB-500 or KLOW-like blends are not treated as one peptide. |
- Is there a clear injury diagnosis and rehab plan?
- Is the goal local tissue support, gut-recovery overlap, or nonspecific pain relief?
- Would imaging, procedure history, or red-flag symptoms change the decision?
- Is there active cancer history, infection concern, autoimmune context, pregnancy context, or tested-sport relevance?
- Can benefit or side effects be attributed if BPC-157 is blended with other compounds?
- Clinical interpretation by injury type, rehab phase, and functional goal.
- Whether the discussion centers on local tissue injury, gut overlap, or post-procedure context.
- Monitoring emphasis based on pain behavior, swelling, procedures, and training load.
- The absence of an approved human healing label.
- FDA safety-risk concerns around immunogenicity, peptide impurities, and API characterization.
- Cancer, infection, surgery, pregnancy, and red-flag injury review.
- Treating blends or research-only products as equivalent to an evaluated medication.
- Converting internet protocols into vial or syringe instructions.
Administration literacy for BPC-157 is mainly about boundaries. The Blueprint does not translate research or community practice into injection instructions.
- Confirm the exact compound identity and product context before interpreting any external claim.
- Do not infer route, frequency, or exposure from vendor language.
- Avoid mixing BPC-157 with TB-500, GHK-Cu, or KLOW-like blends when the goal is to understand causality.
- Post-surgical, infection-prone, or unexplained pain contexts need clinician review before any peptide discussion.
BPC-157 should be read as an adjunct discussion around recovery, not as the maintenance plan itself.
- Rehab progression, load management, sleep, protein, and diagnosis remain the core recovery plan.
- If function improves, do not remove the rehab foundation and assume the compound solved the tissue issue.
- If function does not improve, reassess diagnosis and load instead of adding more recovery peptides.
| Question | Reference answer |
|---|---|
| Is BPC-157 an approved injury-healing drug? | No. This dossier treats it as research-sensitive recovery context, not an approved human healing label. |
| Can the report tell me how many applications to use? | No. There is no universal official schedule here, and the report does not publish application counts. |
| Is a BPC-157 plus TB-500 blend the same evidence? | No. A blend changes attribution, safety interpretation, and quality risk. |
| What decides whether it fits recovery? | Diagnosis, rehab status, injury age, functional limitation, safety context, and whether the claim is supported by reliable sources. |
Educational reference only. BPC-157 does not have a universal approved human recovery protocol in this report.
- Do not treat BPC-157 as a proven tendon cure.
- Do not replace rehab or imaging with peptide use.
- Do not copy vial or syringe conversions from forums.
- Do not turn a blend into a single evidence-backed product.
Monitoring and labs
- Clarify diagnosis, injury type, injury age, location, imaging status, rehab plan, and current load-management strategy.
- Record pain at rest, pain during load, pain 24 hours after training, range of motion, strength, swelling, and training tolerance.
- Document return-to-run, return-to-squat, or return-to-sport markers when relevant.
- Record sleep impact, protein/nutrition context, rehab adherence, and medication changes.
- Review medications, procedures, autoimmune history, cancer history, pregnancy context, and tested-sport status.
- Track function, pain at rest, pain under load, next-day pain, training load, swelling, local irritation, systemic symptoms, and whether rehab tolerance actually improves.
- Separate normal loading adaptation from a peptide-attributed effect.
- Pause interpretation if multiple new compounds or blends were introduced together.
- Escalate medical review if new red-flag symptoms appear.
- Keep progressive loading, sleep, protein adequacy, and recurrence prevention as the foundation.
- Reassess if pain returns, function stalls, or the compound becomes a substitute for diagnosis or rehab.
- Use functional milestones rather than calendar promises to judge return-to-run, return-to-squat, or return-to-sport readiness.
- Treat stopping as an interpretation checkpoint, not as a universal taper.
Recovery monitoring is functional: pain behavior, load tolerance, tissue response, rehab adherence, and safety signals matter more than scale-style metrics.
Regulatory status & study stage
BPC-157 is not approved by FDA as a tendon, ligament, surgery, gut, pain, or sports-recovery medication. FDA safety-risk materials should frame how compounding and research-only claims are read.
| Item | Status | How to read it |
|---|---|---|
| FDA label | No approved recovery label | No branded human healing indication is used as an anchor. |
| FDA safety-risk page | Compounding concern | BPC-157 is listed among withdrawn category-2 nominations with immunogenicity and API characterization concerns. |
| Evidence stage | Preclinical-heavy | Human translation is limited and not adequate for a universal protocol. |
- Mechanistic and animal literature is broad.
- Human efficacy evidence remains limited.
- The current Peptivius role is education and cautious comparison.
- Research-only and grey-market access should not be treated as clinical approval.
- Compounded-product claims need regulatory and quality review.
- Anecdotal popularity does not remove diagnosis, rehab, or safety requirements.
The regulatory frame is deliberately conservative because recovery claims are easy to overread.
Stacking and synergies
BPC-157 appears often in recovery stacks, but this dossier evaluates it individually. Niche-level combination literacy appears in the final conclusion.
- Physical therapy, progressive loading, sleep, protein, and diagnosis are the most defensible support foundation.
- Procedure or wound-care plans should follow professional instructions.
- Gut-recovery context can be discussed separately if symptoms justify it.
- BPC-157 plus TB-500 when causality is the goal.
- KLOW-like all-in-one blends treated as cleaner evidence.
- Multiple repair peptides added before diagnosis is clear.
- Post-surgical recovery.
- Active infection, malignancy history, pregnancy, or severe injury.
- Competitive athletes subject to testing.
Do not add more repair peptides to compensate for unclear diagnosis or poor rehab structure.
Genetic variable
No validated consumer genetic marker determines BPC-157 response. Future tendon, collagen, inflammation, and wound-healing genetics may help frame risk, but they should not be used as a dosing or selection engine now.
- General connective-tissue and inflammation genetics can contextualize injury risk, not BPC response.
- Angiogenesis and collagen-remodeling pathways overlap with BPC-157 mechanisms.
- No SNP should be used to predict BPC-157 benefit.
Genetics may explain vulnerability to injury better than response to a research peptide.
Real-world reports
- Strong anecdotal interest around tendon, ligament, joint, and gut recovery.
- Users often report faster comfort or training tolerance, but attribution is difficult.
- Blends with TB-500 are common in community discussion.
- Regulatory and quality concerns.
- No clear injury diagnosis.
- Lack of obvious functional improvement.
- Concern about cancer history, procedures, or infection.
- Real-world reports explain interest, not proof.
- The useful question is functional change under a stable rehab plan.
- Anecdotes should not override FDA safety-risk framing or human-evidence gaps.
Final personalized interpretation
For Ana, BPC-157 earns the highest Recovery rank because the main recovery signal is chronic patellar tendinopathy, not generic fatigue. The peptide's recovery narrative maps to localized tissue support better than the other compounds in this niche.
The caution is equally important: Ana's knee issue still needs load management, rehab progression, symptom tracking, and diagnosis clarity. BPC-157 should not become a shortcut around those foundations.
The practical interpretation is a high-interest discussion point for a licensed professional, with conservative expectations and no blend-first thinking.
For Ana, BPC-157 is the clearest Recovery match, but only inside a structured rehab and safety-review frame.