Tirzepatide
One of the strongest peptide options for appetite, weight loss, and metabolic health.
Dual GLP-1 and GIP receptor agonist, administered once weekly by subcutaneous injection.
Tirzepatide acts on pathways tied to hunger, satiety, insulin response, and metabolic regulation. It can support sustained weight loss, but the fit depends on GI tolerance, protein intake, training continuity, and lean-mass preservation.
Why it may make sense for you
In Ana's case, tirzepatide appears at the top because the profile combines strong signals of elevated appetite, difficulty with sustained fat loss, and metabolic risk.
| Signal | Interpretation |
|---|---|
| Declared objective | Significant weight loss |
| Hunger pattern | Elevated appetite / food noise |
| Metabolism | Insulin resistance or metabolic risk |
| Tolerance | Needs careful titration |
| Lean mass | Needs protein and resistance-training strategy |
- High potency for appetite reduction
- Strong evidence for clinically meaningful weight loss
- Can be relevant in profiles with insulin resistance
- Weekly use can simplify adherence
- GI effects are common during escalation
- Rapid loss can reduce lean mass without a plan
- Pancreatitis history, MTC/MEN2, pregnancy, or lactation require caution or contraindication review
- People using glucose-lowering medication need professional monitoring
How it works
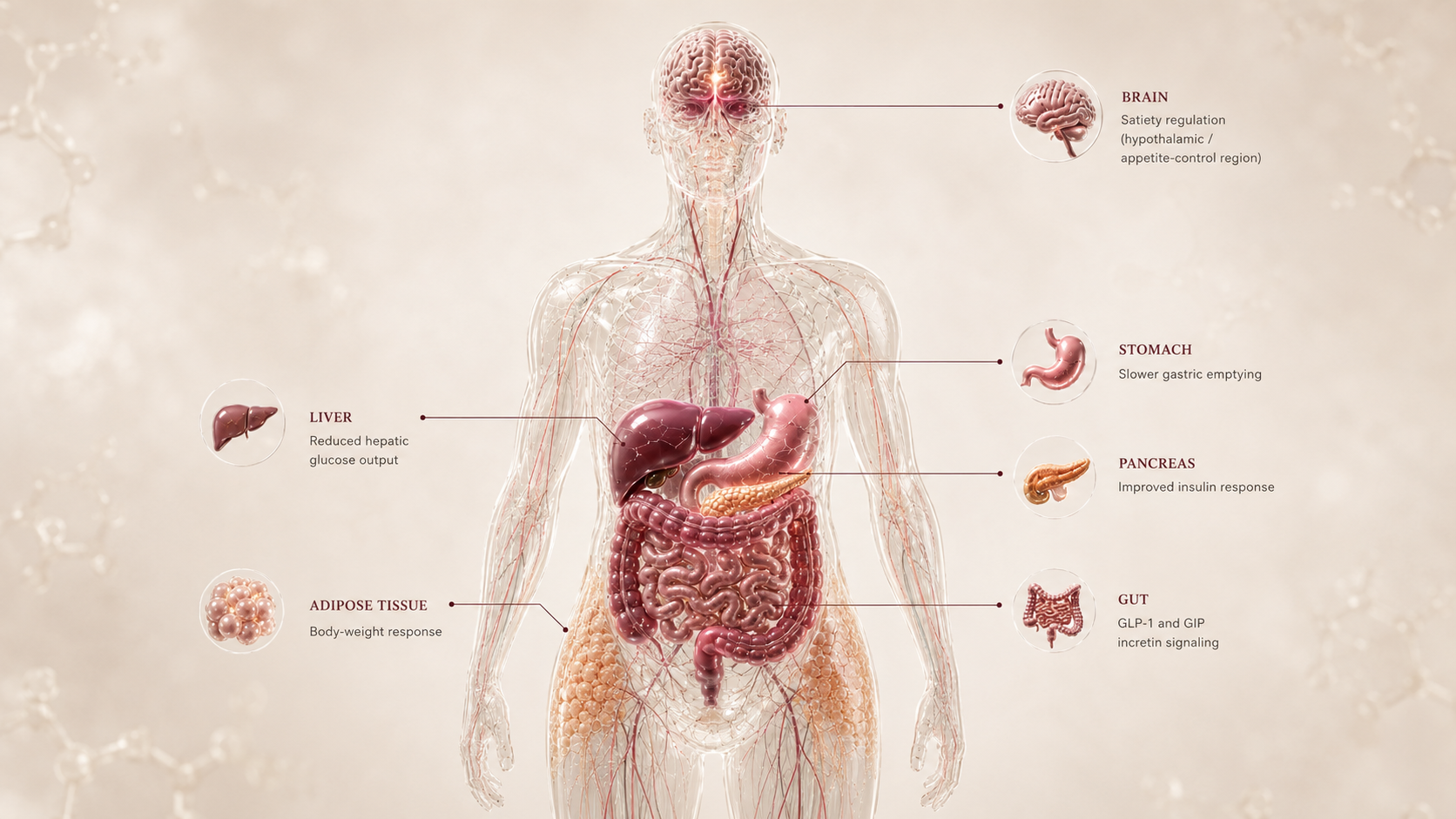
Tirzepatide activates two hormone pathways involved in hunger, satiety, glucose handling, and metabolic response: GLP-1 and GIP. In practical terms, that can reduce food noise, increase fullness after meals, improve insulin response, and make sustained calorie reduction more realistic.
| Pathway | Practical effect |
|---|---|
| Brain | Less food noise |
| Stomach | Slower gastric emptying |
| Pancreas | Better insulin response |
| Body | Greater chance of sustained weight loss |
Less hunger, more satiety, better glycemic control, and a stronger chance of real weight loss.
What the evidence shows
Tirzepatide has one of the strongest clinical evidence bases in the Weight Loss niche. The studies show meaningful weight loss, metabolic improvement, and strong performance in some comparisons against earlier incretin therapies.
| Study | Population | Key result | How to read it |
|---|---|---|---|
| SURMOUNT-1 | Adults with obesity or overweight | Substantial mean weight loss over 72 weeks | Shows high efficacy for sustained weight loss |
| SURPASS / type 2 diabetes studies | People with type 2 diabetes | HbA1c improvement with weight reduction | Relevant for metabolic-risk profiles |
| Comparisons with semaglutide | Obesity, overweight, or diabetes populations | Trend toward greater weight loss in some analyses | Helps explain when tirzepatide may outperform GLP-1-only therapy |
- Individual results vary
- Adherence and tolerance determine continuity
- Maintenance after stopping still needs strategy
- Long-term success depends on monitoring and habits
Safety, side effects, and contraindications
- Nausea
- Constipation or diarrhea
- Gastrointestinal discomfort
- Reflux
- Reduced appetite
- Temporary fatigue
- Pancreatitis, although rare
- Gallbladder issues
- Dehydration
- Acute kidney injury risk during volume depletion
- Pulmonary aspiration risk disclosure before general anesthesia or deep sedation
- Oral contraceptive absorption concerns during initiation and escalation
- Lean-mass loss
- Low protein intake
- Difficulty maintaining training during titration
- Personal or family history of medullary thyroid carcinoma
- MEN2
- Prior pancreatitis
- Pregnancy or lactation
- Active or relevant history of eating disorder
- Use of multiple glucose-lowering medications
- Planned procedures or surgeries requiring delayed-gastric-emptying disclosure
For Ana, the critical point is not only losing weight. It is losing weight while protecting lean mass, digestive tolerance, and regular nutrition.
Reference protocol
FDA label anchor: Zepbound chronic weight-management labeling is the primary anchor. Mounjaro is a diabetes label and is not automatically the same indication.
- Mounjaro used as if it were the Zepbound weight-management label
- Compounded tirzepatide vials or multi-dose products
- Research-only tirzepatide
- Semaglutide or other GLP-1-only labels
- Community dose charts or syringe-unit conversions
| Item | Reference |
|---|---|
| Label ladder | Zepbound labeling describes 2.5 mg once weekly for initiation, then 5 mg, with possible 2.5 mg increases after at least 4 weeks; weight-reduction maintenance is 5 mg, 10 mg, or 15 mg weekly. This is label context, not a personal dose. |
| Application footprint | Weekly injection framing: roughly 4 administrations per 28 days. |
| Route | Subcutaneous injection in the Zepbound/Mounjaro-style label context. |
| Time to maintenance | Maintenance selection depends on response and tolerability after the escalation period; the initiation dose is not a maintenance dose. |
| Decision points | GI tolerance, appetite response, glucose markers, nutrition adequacy, body composition, medication review, oral contraceptive context, procedure disclosure, and access. |
- The initiation step is for adaptation, not a maintenance destination.
- Food-noise reduction can appear early, but tolerability and nutrition decide whether the path is usable.
- The label uses staged weekly dosing with at least 4 weeks on a step before considering an increase.
- Escalation is not automatic; response and tolerability decide whether a step is reasonable.
- Track appetite, GI symptoms, hydration, protein, training continuity, glucose markers, and body composition.
- Rapid scale change without nutrition adequacy can weaken the long-term result.
- Maintenance is label-defined around ongoing weight reduction and long-term weight management.
- Lean mass, protein intake, and resistance training are part of the maintenance interpretation.
- Plateau should trigger a review of dose history, adherence, nutrition, symptoms, access, sleep, and training.
- Stopping should be treated as a maintenance plan because withdrawal studies show regain risk.
| Item | Reference |
|---|---|
| Initial reference dose | 2.5 mg weekly |
| Titration | Gradual increase according to tolerance |
| Frequency | Once weekly |
| Route | Subcutaneous |
| Typical duration | Continuous use with periodic reassessment |
| Decision points | Tolerance, response, labs, protein intake, and body composition |
- Is the current dose tolerated well enough to continue the label path?
- Is the user losing weight while preserving protein intake and resistance training?
- Are glucose-lowering medications, thyroid history, pancreatitis history, pregnancy, or eating-disorder context present?
- Are oral hormonal contraceptives or other oral medications affected by delayed gastric emptying?
- Is a surgery or procedure planned where delayed gastric emptying must be disclosed?
- Does a plateau require maintenance review, not immediate stacking?
- Maintenance dose selection within the official label based on response and tolerability.
- Whether escalation pauses when GI symptoms, intake collapse, or dehydration appear.
- Follow-up cadence based on labs, medications, access, and body-composition trend.
- Whether tirzepatide is used as first incretin path or after prior semaglutide exposure.
- Zepbound versus Mounjaro indication boundaries.
- Contraindication review for MTC/MEN2, pancreatitis history, pregnancy, and serious hypersensitivity.
- Oral contraceptive counseling, kidney risk during volume depletion, gallbladder/pancreatitis review, and procedure/anesthesia disclosure.
- Treating compounded or research-only products as equivalent to FDA-approved branded medication.
- Converting mg into syringe units from generic internet charts.
- Combining with another incretin or strong appetite suppressant without professional review.
Administration literacy should follow the exact product label and presentation. The Blueprint does not translate branded dosing into non-label vial, multi-dose, or insulin-syringe instructions.
- Confirm whether the reference is Zepbound, Mounjaro, a vial, a pen, or another presentation before interpreting dose language.
- Use product-specific missed-dose, storage, device, and syringe instructions from the label or clinician.
- Delayed gastric emptying can matter for oral medications, oral hormonal contraception, and planned procedures.
- Do not split pens, improvise component conversions, or stack with another incretin to imitate a different product.
Tirzepatide is a chronic weight-management context. The off-ramp question is maintenance planning, not a universal taper.
- Plan for appetite return, food-noise return, access continuity, and nutrition/training preservation before stopping.
- Review weight trend, waist, labs, lean mass, and symptoms before deciding whether to hold, change, or transition.
- SURMOUNT-4 showed that withdrawing tirzepatide after weight loss led to substantial regain compared with continued treatment.
| Question | Reference answer |
|---|---|
| How many applications per month? | Weekly injection framing is about 4 administrations per 28 days. |
| How long until maintenance? | The Zepbound label uses at least 4 weeks per escalation step, then maintenance dose selection based on response and tolerability. |
| Is 2.5 mg a maintenance dose? | In the Zepbound label, 2.5 mg is the initiation dose and is not a maintenance dose. |
| Can a compounded vial be read like Zepbound? | No. FDA-approved branded products and compounded or research-only products are not interchangeable references. |
| Is there a universal taper? | No universal taper is defined here. The relevant question is maintenance and discontinuation planning with a professional. |
Educational reference based on public prescribing patterns and literature. This is not a prescription.
- Do not escalate dose quickly without a clear reason
- Do not ignore persistent GI effects
- Do not combine with other incretins without professional review
- Do not treat scale weight as the only success marker
Monitoring and labs
- Weight and waist circumference
- Body composition, if available
- Fasting glucose
- HbA1c
- Lipid profile
- Liver function
- Kidney function
- Thyroid history
- Current medications
- GI tolerance
- Hydration
- Protein intake
- Glucose response
- Weight trend
- Energy and training
- Persistent symptoms
- Body composition
- Lean mass
- Nutrition plan
- Appetite control
- Metabolic labs
- Maintenance strategy
The goal is not just lowering the scale number. It is tracking response, safety, and sustainability.
Regulatory status & study stage
Tirzepatide is not a research-only peptide in its approved indications. It is the active drug behind Mounjaro and Zepbound, with FDA-approved uses in type 2 diabetes and chronic weight management.
| Item | Status | How to read it |
|---|---|---|
| Mounjaro | FDA approved for type 2 diabetes | Original approval was May 13, 2022. This is the diabetes indication for the same active drug. |
| Zepbound | FDA approved for chronic weight management | Approved on Nov 8, 2023 for eligible adults with obesity or overweight with at least one weight-related condition. |
| Study stage | Approved drug with ongoing research | The core indications are no longer experimental, but post-market and expanded-indication studies still matter. |
- Approved medication in specific indications, not a research-only molecule in those contexts.
- Supported by large Phase 3 obesity and diabetes programs.
- Ongoing studies can expand indications, compare against newer agents, and refine long-term safety.
- A branded prescription pathway exists through Mounjaro and Zepbound.
- Cost, insurance coverage, country, supply, and prescriber criteria can change practical access.
- Compounded, research-only, or grey-market products should not be treated as equivalent to FDA-approved branded medication.
Approval is indication-specific. It does not make compounded, research-only, or grey-market products equivalent to FDA-approved branded medication.
Stacking and synergies
Combinations should be read as an educational compatibility and risk map, not as a recommendation to use a stack.
- Tirzepatide plus protein strategy and resistance training
- Tirzepatide plus body-composition monitoring
- Tirzepatide plus metabolic support in selected profiles
- Two GLP-1 or incretin agents at the same time
- Tirzepatide plus another strong appetite suppressant without a clear reason
- Glucose-lowering medications
- Insulin
- Other incretin agents
- Aggressive weight-loss protocols
- GH-axis peptides when metabolic risk or sleep apnea is present
Avoid starting multiple compounds at the same time. It makes benefits, side effects, and causality harder to understand.
Genetic variable
Some genetic differences may influence appetite, satiety, GLP-1/GIP response, and tendency toward insulin resistance. Genetics does not determine response by itself, but it can calibrate expectations.
- Metabolic and appetite pathways can influence baseline risk and response context
- A future genetic layer may adjust expectation, caution, and follow-up intensity
- No single SNP should be treated as a deterministic response rule
Genetics should calibrate expectation, not replace clinical evaluation or monitoring.
Real-world reports
- Reduced food noise
- Less drive toward sweets
- Faster satiety
- Difficulty hitting protein
- Nausea or constipation during titration
- Cost
- Gastrointestinal effects
- Reduced pleasure from eating
- Plateau
- Regain after stopping without a plan
- Reports are qualitative data, not clinical evidence
- Placebo effects, selection bias, and cointerventions exist
- They help calibrate expectations, not decide use
Final personalized interpretation
For Ana, tirzepatide ranks highly because the profile is not only about lowering body weight. The onboarding pattern points to elevated appetite pressure, food-noise friction, prior semaglutide exposure, PCOS, metformin use, and a plateau with concern about muscle tone. That combination makes the match stronger than a generic weight-loss preference would suggest.
The strongest argument is the overlap between tirzepatide's appetite and metabolic evidence and Ana's declared problem: sustained weight loss with metabolic resistance in the background. A dual GLP-1/GIP pathway is relevant because the profile is not just about willpower or routine. It is about satiety, insulin response, hunger signaling, and whether the plan can remain consistent long enough to matter.
The main caution is that a strong weight-loss signal can create its own problems if the plan is not structured. In Ana's case, the critical watchpoint is losing weight while preserving lean mass, protein intake, resistance training, hydration, and regular eating rhythm. GI tolerance is not a side detail here; it determines whether the intervention remains usable.
Regulatory status also changes the interpretation. Tirzepatide is not a research-only peptide in its approved indications, which gives it a different evidence and access profile than pipeline compounds. But approval is not the same as automatic fit. Contraindications, medication context, cost, access, monitoring, and professional review still decide whether this path makes sense in Ana's real situation.
The practical conclusion is a high-fit option to discuss with a licensed professional, not a standalone recommendation. The Match Score explains why tirzepatide belongs near the top; the full decision depends on whether Ana can pair it with the monitoring, nutrition, training, and safety review needed to make the result sustainable.