Tesamorelin
A niche body-composition peptide, most relevant when visceral abdominal fat is the target.
Growth-hormone-releasing hormone analog administered by subcutaneous injection in approved contexts for excess abdominal fat in HIV-associated lipodystrophy.
Tesamorelin is not a broad appetite suppressant and is not approved as general weight-loss management. Its relevance comes from GH/IGF-1 signaling and a specific approved context for excess abdominal fat in HIV-associated lipodystrophy.
Why it may make sense for you
For Ana, tesamorelin appears as a secondary Weight Loss option because the profile includes body-composition concerns, but the main stated pattern is better served by appetite and metabolic incretin pathways.
| Signal | Interpretation |
|---|---|
| Declared objective | Body recomposition matters |
| Primary mismatch | Not an appetite-first compound |
| Metabolic context | Glucose/IGF-1 awareness is important |
| Potential relevance | Abdominal adiposity and body-composition nuance |
| Rank reason | Narrower use-case than incretins |
- May be relevant if visceral fat is a specific concern.
- Body-composition framing fits part of Ana's stated problem.
- Useful contrast against appetite-centered agents.
- Approved indication gives it more maturity than many GH-axis peptides.
- Does not directly solve food noise.
- Not the best match for broad weight-loss initiation.
- Glucose and IGF-1 context need review.
- Higher complexity and narrower clinical fit reduce ranking.
How it works
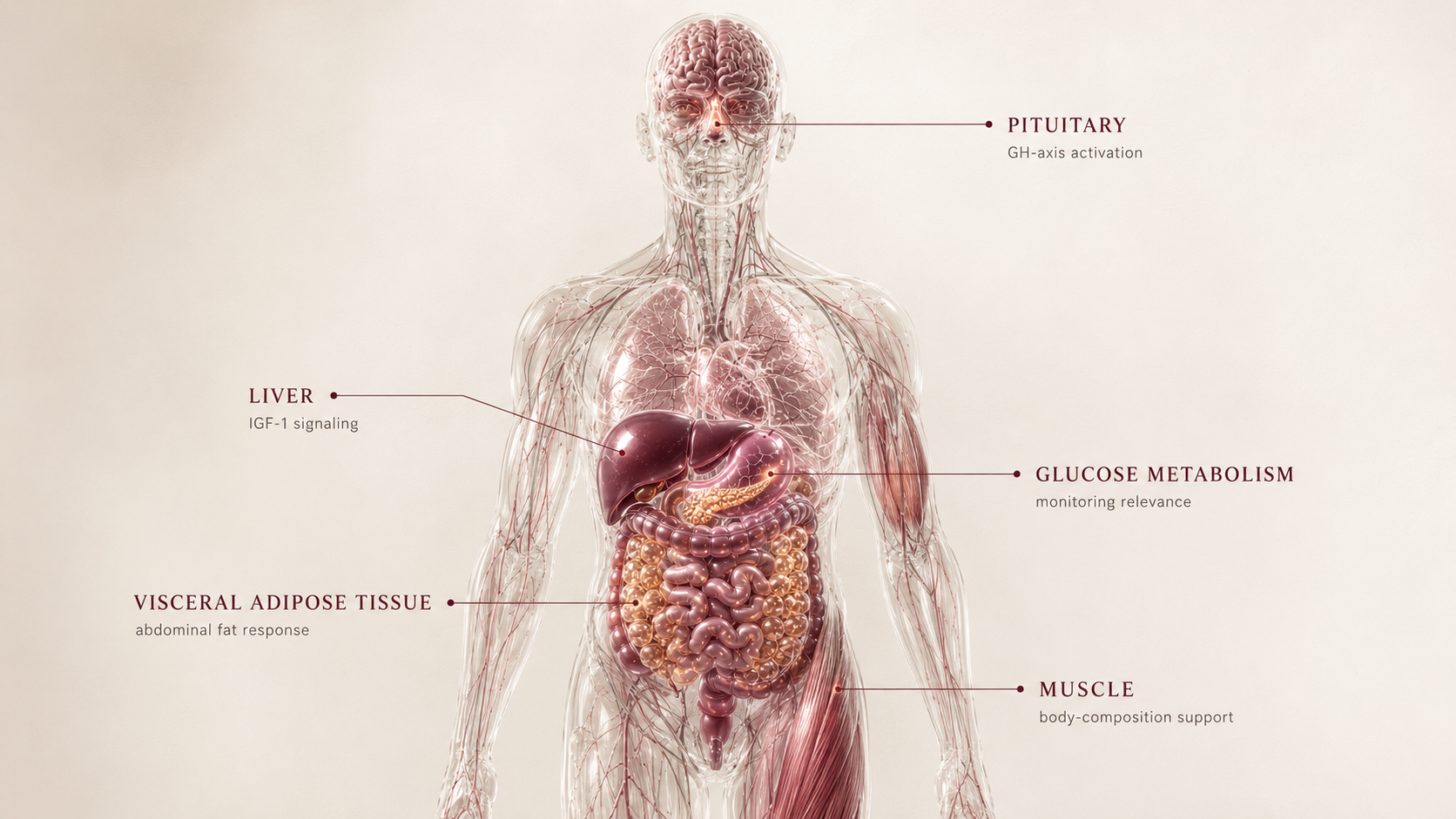
Tesamorelin stimulates growth-hormone-releasing hormone signaling, increasing endogenous GH pulse activity and downstream IGF-1 exposure. In weight-loss framing, its relevance is indirect: abdominal fat distribution and body composition rather than appetite suppression.
| Pathway | Practical effect |
|---|---|
| Pituitary | Stimulates GH release |
| Liver/tissues | Increases IGF-1 signaling |
| Adipose context | Targets visceral-fat relevance in approved indication |
| Body composition | Indirect support rather than appetite control |
Tesamorelin is more about visceral fat and GH-axis signaling than hunger, cravings, or food noise.
What the evidence shows
Tesamorelin has evidence in a narrower approved context: reducing excess abdominal fat in adults with HIV-associated lipodystrophy. That evidence does not automatically translate into general weight-loss use.
| Study | Population | Key result | How to read it |
|---|---|---|---|
| Tesamorelin HIV-lipodystrophy studies | Adults with excess abdominal fat in HIV-associated lipodystrophy | Reduction in visceral adipose tissue in the approved context | Strong for a narrow indication, not broad obesity treatment |
| GH/IGF-1 monitoring literature | GH-axis clinical contexts | Shows why IGF-1 and glucose awareness matter | Safety and monitoring are central to interpretation |
| Weight Loss category comparison | General body-composition goals | Less direct than GLP-1/GIP appetite agents | Explains lower ranking for Ana's stated profile |
- General weight-loss translation is limited.
- Individual visceral-fat response varies.
- Long-term body-composition strategy still matters.
- Metabolic context changes risk/benefit interpretation.
Safety, side effects, and contraindications
- Injection-site reactions
- Joint or muscle discomfort
- Fluid retention
- Tingling or numbness
- Headache
- IGF-1 elevation
- Glucose intolerance risk
- Edema or carpal-tunnel-like symptoms
- Cancer-history review in GH-axis contexts
- Not suitable as an unsupervised body-composition shortcut
- Active malignancy or relevant cancer-history review
- Pregnancy
- Hypersensitivity to tesamorelin or related components
- Pituitary-axis conditions requiring specialist review
- Diabetes or glucose dysregulation requires caution
For Ana, the main issue is that tesamorelin may speak to body composition, but it does not directly address the appetite and food-noise pressure that drives the Weight Loss ranking.
Reference protocol
Adjacent indication anchor: Egrifta SV/WR tesamorelin labeling is anchored to excess abdominal fat in HIV-associated lipodystrophy, not broad weight-loss treatment.
- A general obesity or appetite-control label
- Sermorelin or other GH secretagogues
- Research-only tesamorelin
- Compounded GH-axis stacks
- Broad visceral-fat marketing claims outside the approved context
| Item | Reference |
|---|---|
| Reference framing | Approved indication is narrow: excess abdominal fat in HIV-associated lipodystrophy. |
| Frequency | Daily subcutaneous use in the approved medication context. |
| Application footprint | Daily framing: about 30 administrations per month. |
| Formulation caution | Egrifta formulations have product-specific preparation, dose, and storage instructions. |
| Decision points | IGF-1, glucose, cancer-history review, abdominal adiposity, edema, symptom burden, and specialist oversight. |
- First question: is the user discussing the approved indication or a broader body-composition extrapolation?
- Weight Loss relevance is indirect and should not be framed as appetite control.
- IGF-1, glucose markers, body composition, abdominal-fat context, and cancer-history review matter before interpretation.
- The GH-axis makes this a higher-monitoring conversation.
- Monitor injection-site tolerance, edema, joint symptoms, glucose response, and whether the use-case remains specific enough.
- Do not judge fit by scale weight alone.
- Continuation depends on measurable body-composition relevance and tolerability.
- A weak appetite effect is expected because this is not an appetite peptide.
- If the goal is food noise or broad weight loss, redirect to better-fit incretin comparisons.
- If monitoring burden outweighs benefit, the compound should remain secondary.
| Item | Reference |
|---|---|
| Reference framing | Daily subcutaneous use in approved indication |
| Route | Subcutaneous |
| Frequency | Daily in approved medication context |
| Decision points | IGF-1, glucose, abdominal adiposity, contraindications, and specialist oversight |
| Use-case | Visceral fat/body-composition context, not broad appetite control |
- Is the goal visceral adiposity/body composition or general appetite control?
- Is the user eligible for the approved indication context or extrapolating beyond it?
- Are IGF-1, glucose, edema, and cancer-history review accounted for?
- Does daily administration fit the user's adherence reality?
- Would a lower-complexity incretin answer the actual Weight Loss problem better?
- How clinicians judge adjacent body-composition relevance outside the narrow indication.
- Follow-up cadence based on IGF-1, glucose, symptoms, and body-composition data.
- Whether the compound belongs in Weight Loss or another niche for a given user.
- Access practicality by country, product, coverage, and indication fit.
- The approved-indication boundary.
- Product-specific preparation and storage instructions.
- IGF-1 and glucose monitoring expectations.
- Cancer-history and pituitary/endocrine review.
- Assuming all GH-axis peptides are interchangeable.
Tesamorelin administration must be read through the specific approved product instructions. The Blueprint does not generalize Egrifta handling to compounded or research-only GH-axis products.
- Confirm formulation before interpreting preparation or storage details.
- Do not translate one Egrifta formulation's handling into another formulation or research product.
- Daily administration increases operational burden compared with weekly incretins.
Maintenance means deciding whether the narrow body-composition signal justifies ongoing GH-axis monitoring, not chasing scale loss.
- Reassess body-composition relevance, IGF-1, glucose, edema, and symptom burden.
- If appetite is still the bottleneck, tesamorelin is probably the wrong Weight Loss lever.
- Stopping or redirecting should be based on whether the narrow indication logic still holds.
| Question | Reference answer |
|---|---|
| Is this a broad fat-loss peptide? | No. The anchor is a narrow approved indication, not general obesity treatment. |
| How many applications per month? | Daily framing is about 30 administrations per month in approved medication context. |
| Does it reduce food noise? | That is not the primary mechanism. It is not an appetite-first peptide. |
| Why is monitoring heavier? | GH/IGF-1 signaling intersects with glucose, edema, and endocrine safety context. |
| Can it replace GLP-1/GIP options? | Not for appetite-driven Weight Loss. It is a narrower body-composition discussion. |
Educational reference only. Tesamorelin's approved use is indication-specific and this is not a prescription.
- Do not treat tesamorelin as a general appetite suppressant.
- Do not ignore IGF-1 or glucose monitoring.
- Do not use GH-axis logic without cancer-history and metabolic review.
- Do not stack with other GH-axis agents casually.
Monitoring and labs
- Waist and abdominal-fat context
- Body composition if available
- Fasting glucose and HbA1c
- IGF-1
- Cancer-history review
- Medication review
- IGF-1 trend
- Glucose response
- Edema or joint symptoms
- Injection-site tolerance
- Abdominal composition trend
- Visceral-fat response if measured
- Metabolic labs
- Symptom burden
- Whether benefit matches the narrow use-case
Monitoring should determine whether the body-composition signal is specific enough to justify the complexity.
Regulatory status & study stage
Tesamorelin is FDA approved in a specific indication related to excess abdominal fat in HIV-associated lipodystrophy. That does not make it a general obesity medication.
| Item | Status | How to read it |
|---|---|---|
| Egrifta / tesamorelin | FDA approved in a defined indication | Most relevant to visceral abdominal fat in HIV-associated lipodystrophy. |
| Weight Loss use | Contextual / not broad appetite medicine | Use-case is narrower than GLP-1 and incretin therapies. |
| Study maturity | Mature in narrow indication | General body-composition extrapolation should be conservative. |
- Approved medication in a narrow indication.
- Evidence is strongest for visceral adipose tissue in that context.
- Not a mature broad-obesity treatment category.
- Prescription pathway exists in the approved indication.
- Coverage and use-case fit can be restrictive.
- Research-only or compounded sources should not be treated as equivalent.
Approval is indication-specific. It does not convert tesamorelin into a general-purpose weight-loss medication.
Stacking and synergies
Tesamorelin combinations should be read through GH-axis complexity, not appetite stacking.
- Tesamorelin plus body-composition monitoring.
- Tesamorelin plus resistance training and protein adequacy.
- Tesamorelin plus glucose and IGF-1 tracking.
- Tesamorelin plus other GH secretagogues without professional review.
- Tesamorelin used as a substitute for appetite-centered therapy.
- Diabetes or prediabetes
- Cancer history
- Sleep apnea risk
- GH-axis medications or peptides
- Edema or carpal tunnel symptoms
Do not stack GH-axis compounds casually; overlapping mechanisms can obscure both benefit and risk.
Genetic variable
Genetic context for tesamorelin is less direct than for appetite-centered incretins. Future DNA layers may help interpret GH/IGF signaling, insulin sensitivity, and body-fat distribution.
- Insulin and adiposity-related genetics can shape metabolic baseline.
- GH/IGF-axis variants may become useful context for response expectations.
- No genetic marker should be used to claim tesamorelin weight-loss response.
For this peptide, labs and indication fit matter more than genetics in Slice 1.
Real-world reports
- Interest in abdominal fat reduction
- Body-composition framing rather than appetite suppression
- Concern about cost and access
- Questions around IGF-1 and glucose
- Confusion with general GH secretagogues
- Narrow use-case
- Daily administration
- Cost
- Monitoring burden
- Limited appetite effect
- Real-world interest often overgeneralizes the approved indication.
- It should be judged against visceral/body-composition goals, not food noise.
- Anecdotes do not expand the label or evidence base.
Final personalized interpretation
For Ana, tesamorelin is relevant because the onboarding does not only mention scale weight. It also includes body-composition and muscle-tone concerns, which makes a visceral/body-composition peptide worth explaining.
The reason it ranks well below the incretins is that Ana's strongest Weight Loss signal is appetite and metabolic friction, not a narrowly defined visceral-fat indication. Tesamorelin does not directly address food noise in the way GLP-1/GIP pathways can.
The monitoring burden also matters. PCOS and metformin use keep glucose context in the foreground, and GH-axis compounds require more attention to IGF-1, glucose, edema, and symptom response.
So the practical read is contextual: tesamorelin can be part of the body-composition map, but it should not distract from the higher-fit appetite and metabolic options.
For Ana, tesamorelin is a secondary discussion point, not the lead Weight Loss match.