Sermorelin
A GH-axis peptide that may support body composition indirectly, but is not a primary weight-loss compound.
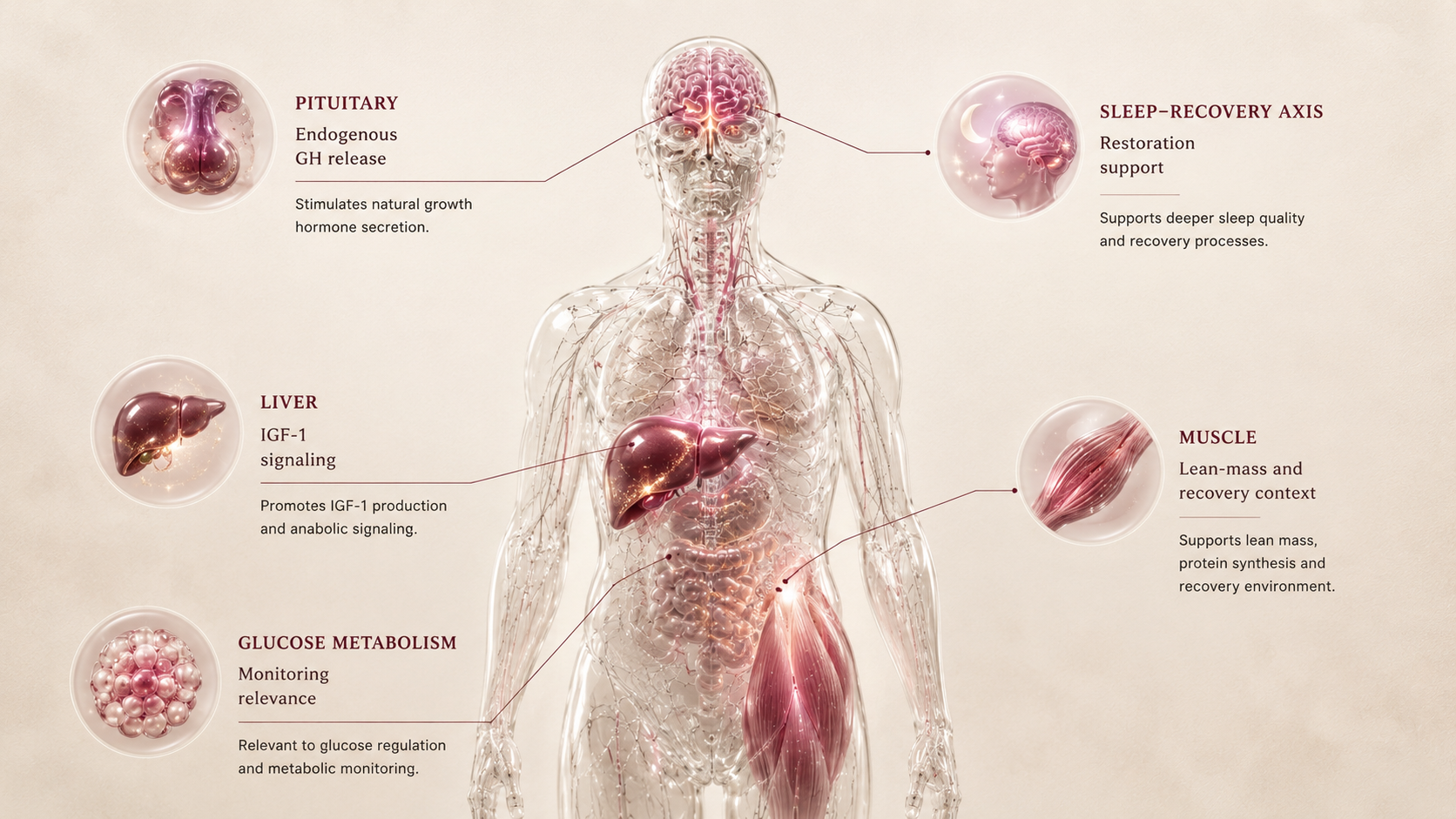
Growth-hormone-releasing hormone fragment that stimulates endogenous GH release through pituitary signaling.
Sermorelin is best understood as a recovery, sleep, or body-composition support signal rather than an appetite or metabolic weight-loss agent. In Weight Loss, it is secondary and contextual.
Why it may make sense for you
For Ana, sermorelin appears only as a secondary Weight Loss option because muscle-tone and recovery concerns exist, but the main Weight Loss problem is appetite and metabolic friction.
| Signal | Interpretation |
|---|---|
| Potential relevance | Lean-mass and recovery context |
| Primary mismatch | Does not directly reduce appetite or food noise |
| Metabolic caution | GH-axis can intersect with glucose context |
| Cross-niche role | More relevant to Recovery or Performance & Muscle |
| Rank reason | Indirect support, weaker weight-loss evidence |
- May support a body-composition conversation.
- Relevant if muscle tone and recovery become primary.
- Could complement lifestyle foundations in supervised contexts.
- Useful to explain why not every Weight Loss peptide is appetite-centered.
- Not a substitute for appetite or metabolic weight-loss agents.
- Glucose and sleep-apnea context need review.
- Evidence is weaker for this niche.
- Should remain secondary in Ana's current ranking.
How it works
Sermorelin stimulates the pituitary to release growth hormone, which can influence IGF-1 and recovery/body-composition pathways. Its Weight Loss relevance is indirect and depends on whether lean mass, sleep, and recovery are the limiting factors.
| Pathway | Practical effect |
|---|---|
| Pituitary | Stimulates GH release |
| Liver/tissues | Supports IGF-1 pathway |
| Recovery | May influence sleep/recovery framing |
| Body composition | Indirect support, not appetite suppression |
Sermorelin is not for food noise. It is a GH-axis support signal that may matter only if body composition and recovery are the bottleneck.
What the evidence shows
Sermorelin has GH-axis relevance, but the evidence for broad Weight Loss use is far weaker than incretin therapies. It belongs in the secondary tier for this niche.
| Study | Population | Key result | How to read it |
|---|---|---|---|
| GH-axis literature | Growth hormone deficiency and related contexts | Shows endocrine pathway relevance | Does not establish it as a primary weight-loss agent |
| Body-composition framing | Recovery and lean-mass support contexts | Indirect relevance to body composition | Useful only when appetite is not the main problem |
| Weight Loss comparison | Incretin vs GH-axis peptides | Weaker direct evidence for weight loss | Explains low ranking in this niche |
- Direct weight-loss effect is not the core evidence base.
- Response depends on GH-axis baseline and monitoring.
- Glucose effects can matter in metabolically sensitive users.
- Compounding quality and access vary.
Safety, side effects, and contraindications
- Injection-site irritation
- Headache
- Flushing
- Dizziness
- Water retention or joint discomfort
- IGF-1 elevation
- Glucose changes
- Edema
- Sleep-apnea risk context
- Carpal-tunnel-like symptoms
- Cancer-history review
- Uncontrolled diabetes or glucose dysregulation requires caution
- Sleep apnea requires review
- Pregnancy or lactation
- Pituitary or endocrine disorders require specialist context
For Ana, sermorelin's main caution is metabolic context: PCOS and metformin make glucose awareness important, while the compound does not directly address appetite pressure.
Reference protocol
Variable clinical context: Sermorelin has GH-axis clinical context but no FDA-approved general weight-loss label. This dossier treats it as secondary body-composition/recovery support.
- A primary obesity medication label
- Tesamorelin's approved HIV-lipodystrophy indication
- A universal compounded protocol
- Other GH secretagogues or secretagogue blends
- Research-only vial instructions
| Item | Reference |
|---|---|
| Reference framing | Variable supervised GH-axis context, not a standardized Weight Loss protocol. |
| Frequency | Not standardized in this Blueprint; clinician and formulation context matter. |
| Application footprint | Cannot be inferred without a specific supervised protocol and product. |
| Route | Often discussed as subcutaneous in supervised contexts, but route alone does not define fit. |
| Decision points | IGF-1, glucose, sleep apnea risk, edema, recovery need, body composition, and cancer-history review. |
- First decide whether the bottleneck is appetite or recovery/body composition.
- If appetite is the main issue, sermorelin is likely a poor Weight Loss lever.
- IGF-1, glucose markers, sleep apnea risk, edema risk, and cancer-history review matter.
- Compounding quality and clinical oversight are part of the context.
- Track sleep, recovery perception, edema, joint symptoms, glucose response, and injection tolerance.
- Do not treat subjective recovery as proof of fat-loss benefit.
- Continuation depends on whether recovery or lean-mass context is measurable and worth the complexity.
- If glucose, edema, or sleep issues worsen, the risk/benefit changes.
- If food noise and metabolic friction remain dominant, redirect to appetite/metabolic comparisons.
- Avoid adding GH-axis complexity just because weight loss has plateaued.
| Item | Reference |
|---|---|
| Reference framing | Usually supervised subcutaneous GH-axis protocol |
| Timing | Often discussed in evening/bedtime contexts |
| Route | Subcutaneous |
| Decision points | IGF-1, glucose, sleep quality, edema, recovery need, and contraindication review |
| Use-case | Body-composition/recovery support, not appetite-first weight loss |
- Is sermorelin being used to answer the wrong problem?
- Are IGF-1, glucose, sleep, edema, and cancer-history context being monitored?
- Is the product compounded, research-only, or clinically supervised?
- Would a simpler appetite-centered option answer the Weight Loss goal better?
- Is the user stacking GH-axis compounds without a clear review path?
- Clinical rationale, schedule, and follow-up in supervised GH-axis care.
- Whether the peptide belongs in Weight Loss, Recovery, Sleep, or Performance & Muscle.
- Monitoring intensity based on glucose, sleep apnea, edema, and IGF-1 context.
- Practical access depending on jurisdiction and compounding oversight.
- Assuming a universal sermorelin protocol exists.
- Skipping glucose, IGF-1, sleep apnea, edema, or cancer-history review.
- Treating sermorelin as equivalent to tesamorelin or stronger GH secretagogues.
- Using research-only vial instructions as clinical guidance.
- Adding GH-axis agents when appetite is the unresolved Weight Loss driver.
Administration cannot be standardized here because sermorelin use depends on clinical context, formulation, and compounding oversight.
- Do not infer syringe units, concentration, or timing from generic peptide guides.
- Confirm formulation and monitoring plan before interpreting any protocol language.
- Route and timing are less important than whether the GH-axis rationale is valid.
Maintenance means proving the compound is solving a real recovery/body-composition bottleneck, not keeping it because it sounds useful.
- Review IGF-1, glucose, edema, sleep, recovery, and body-composition data.
- If benefits are vague, discontinuation or redirection should be discussed.
- Do not use sermorelin as a maintenance substitute for nutrition, resistance training, or appetite strategy.
| Question | Reference answer |
|---|---|
| Is there a standard weight-loss protocol? | No. This dossier does not define a universal sermorelin protocol. |
| How many applications per month? | It cannot be inferred without a specific supervised product and protocol. |
| Is it like tesamorelin? | No. Tesamorelin has a narrow approved indication; sermorelin is a different GH-axis context. |
| Why is it in Weight Loss? | Only because body-composition and recovery can matter indirectly. It is not appetite-first. |
| What is the main safety issue? | GH-axis monitoring: glucose, IGF-1, edema, sleep apnea risk, and cancer-history review. |
Educational reference only. Sermorelin use depends heavily on clinical context, compounding rules, and endocrine monitoring.
- Do not treat sermorelin as a primary fat-loss drug.
- Do not ignore glucose or IGF-1 monitoring.
- Do not combine with other GH-axis agents casually.
- Do not use if sleep apnea or cancer-history context has not been reviewed.
Monitoring and labs
- IGF-1
- Fasting glucose and HbA1c
- Sleep apnea risk
- Body composition
- Cancer-history review
- Medication review
- Sleep quality
- Edema or joint symptoms
- Glucose response
- Recovery perception
- Injection tolerance
- IGF-1 trend
- Lean mass
- Training recovery
- Metabolic labs
- Whether benefit is niche-relevant
The monitoring question is whether GH-axis support is actually relevant to the user's bottleneck.
Regulatory status & study stage
Sermorelin is not an FDA-approved general weight-loss medication. In this Blueprint it is treated as a compoundable/research-sensitive GH-axis peptide with secondary relevance.
| Item | Status | How to read it |
|---|---|---|
| Sermorelin | Compoundable / non-weight-loss framing | Not a branded FDA-approved obesity medication. |
| Study maturity | Endocrine pathway evidence, weak Weight Loss specificity | Mechanism is real, but niche evidence is indirect. |
| Access | Variable compounding and clinical oversight | Quality and regulatory context matter more than popularity. |
- Not a mature broad Weight Loss drug.
- More relevant to GH-axis and body-composition context.
- Evidence is weaker and more indirect than incretin therapies.
- Compounding pathways vary by jurisdiction and provider.
- Research-only products are not equivalent to clinical oversight.
- Professional monitoring is important because GH-axis effects are systemic.
Regulatory and access ambiguity is part of the risk profile, not a side detail.
Stacking and synergies
Sermorelin stacking is mainly a GH-axis question and should stay conservative.
- Sermorelin plus resistance training and recovery tracking.
- Sermorelin plus sleep-quality review.
- Sermorelin plus IGF-1 and glucose monitoring.
- Sermorelin plus other GH secretagogues without professional review.
- Sermorelin used to compensate for poor appetite-control strategy.
- Diabetes or PCOS with glucose concerns
- Sleep apnea
- Cancer history
- Other GH-axis peptides
- Edema or joint symptoms
Avoid adding GH-axis compounds when the unresolved problem is appetite; it can add complexity without addressing the main driver.
Genetic variable
Sermorelin's future genetic layer would likely involve GH receptor signaling, IGF-1 biology, insulin sensitivity, and sleep/circadian context, but this is not a validated response engine today.
- Insulin sensitivity and endocrine baseline shape monitoring needs.
- GH/IGF-axis genetics may eventually calibrate expectations.
- No genetic variant should be used to promise body-composition response.
In Slice 1, BioProfile and labs matter more than genetic speculation for sermorelin.
Real-world reports
- Interest in sleep and recovery
- Body-composition hopes
- Less direct appetite effect
- Confusion with stronger GH secretagogues
- Variable compounding experience
- Weak weight-loss effect
- Monitoring burden
- Cost
- Sleep or edema symptoms
- Unclear benefit
- Reports should be read as recovery/body-composition anecdotes.
- They do not establish sermorelin as a primary Weight Loss compound.
- Benefit claims need to be separated from GH-axis marketing.
Final personalized interpretation
For Ana, sermorelin has one reason to appear in Weight Loss: the profile includes muscle-tone and recomposition concerns, not only scale weight.
That said, the strongest problem pattern is appetite pressure, metabolic friction, prior GLP-1 exposure, and plateau. Sermorelin does not directly solve that pattern.
Its risk/monitoring profile also matters. PCOS and metformin use make glucose awareness important, while GH-axis compounds can add complexity around IGF-1, edema, sleep apnea, and symptom interpretation.
So sermorelin is best read as an adjacent body-composition signal that may belong elsewhere in the Blueprint more than it belongs at the top of Weight Loss.
For Ana, sermorelin is a secondary context peptide, not a primary weight-loss match.