Retatrutide
A next-generation triple agonist with a high metabolic ceiling, but less settled real-world access.
Investigational GLP-1, GIP, and glucagon receptor agonist studied as a once-weekly subcutaneous therapy.
Retatrutide is designed to push beyond GLP-1-only and dual-agonist biology by adding glucagon-pathway activity. That makes it highly relevant to weight-loss research, but current fit depends on study status, tolerability, and practical access.
Why it may make sense for you
For Ana, retatrutide scores well because the profile suggests appetite pressure, metabolic resistance, and a significant weight-loss objective. It stays below approved options because the practical path is less settled and the current Blueprint should prioritize evidence plus real-world usability.
| Signal | Interpretation |
|---|---|
| Declared objective | High-weight-loss ceiling is relevant |
| Metabolic context | PCOS and metformin make metabolic signaling important |
| Peptide experience | Intermediate experience supports understanding complexity |
| Current limitation | Pipeline status reduces practical fit |
| Main watchout | Tolerability and access are less predictable |
- Strong conceptual match for significant weight-loss goals.
- May matter if GLP-1-only response is limited.
- Relevant as a future-category comparison.
- Mechanism fits metabolic-resistance framing.
- Investigational status makes it less practical today.
- Not equivalent to an approved prescription pathway.
- Tolerance and escalation would require careful professional context.
- Long-term real-world pattern is still developing.
How it works
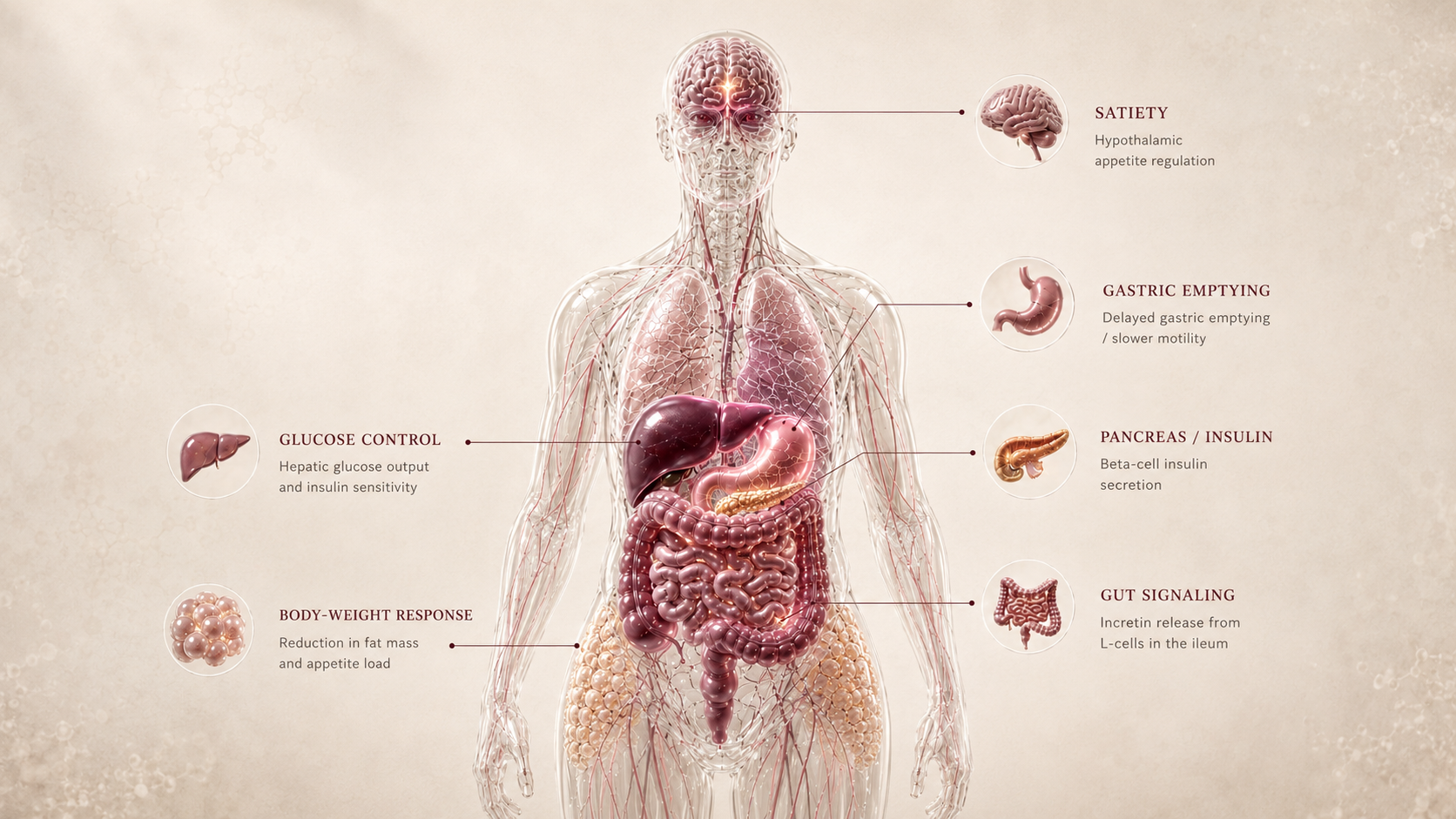
Retatrutide targets three incretin-related pathways: GLP-1 for satiety and glucose response, GIP for metabolic signaling, and glucagon for energy-balance effects. The triple mechanism is why it is watched closely, but it also increases the need for careful interpretation.
| Pathway | Practical effect |
|---|---|
| GLP-1 | Satiety and glucose response |
| GIP | Metabolic signaling support |
| Glucagon | Energy-balance and liver-pathway relevance |
| Whole body | Potentially higher weight-loss ceiling |
Retatrutide is a high-ceiling research signal: more pathways, more potential, and more need for caution.
What the evidence shows
Retatrutide has strong clinical-trial signal for obesity research, but the evidence is not as operationally mature as approved GLP-1 or dual-agonist medications.
| Study | Population | Key result | How to read it |
|---|---|---|---|
| Phase 2 obesity trial | Adults with obesity or overweight | Large weight-loss signal in clinical research | Shows why the compound is a high-ceiling pipeline candidate |
| Phase 3 development | Broader obesity and metabolic populations | Ongoing confirmatory research | Needed before mature approval and access conclusions |
| Comparative category context | Incretin therapies | Triple agonism extends beyond semaglutide and tirzepatide mechanisms | Useful for future ranking, not immediate equivalence |
- Approval status and final labeled indications remain unsettled.
- Long-term safety and maintenance data are less mature.
- Real-world adherence and tolerability remain uncertain.
- Access cannot be treated like an approved branded pathway.
Safety, side effects, and contraindications
- Nausea
- Vomiting or diarrhea
- Constipation
- Reduced appetite
- Injection-site discomfort
- GI burden during escalation
- Dehydration if intake drops sharply
- Lean-mass loss with rapid weight change
- Glucose changes in metabolically sensitive users
- Unknowns typical of pipeline-stage compounds
- Professional review for pancreatitis history
- Professional review for thyroid cancer/MEN2 context
- Pregnancy or lactation
- Active eating disorder history
- Use with glucose-lowering medication requires clinical supervision
For Ana, retatrutide's appeal is its ceiling, but the main caution is that a high-ceiling pipeline compound is not the same as a practical, approved path for a profile already managing metabolic and lean-mass concerns.
Reference protocol
Clinical trial anchor: Retatrutide is anchored to published clinical-trial exposure patterns and active ClinicalTrials.gov programs, not to an approved consumer label.
- An FDA-approved retatrutide dose
- A community retatrutide protocol
- Research-only vials marketed as clinical equivalents
- Compounded retatrutide, which FDA says cannot be used in compounding under federal law
- Semaglutide, tirzepatide, or other approved incretin labels
- Any syringe-unit conversion chart
| Item | Reference |
|---|---|
| Reference framing | Once-weekly subcutaneous retatrutide has been studied in clinical trials. |
| Dose context | Published trials used assigned dose groups and protocol-defined escalation; this is study design, not a consumer protocol. |
| Application footprint | Trial exposure is weekly, but trial visits, eligibility, monitoring, and drug handling are part of the context. |
| Time horizon | The phase 2 obesity trial followed participants for 48 weeks; phase 3 programs use protocol-specific timelines. |
| Decision points | Trial eligibility, investigational status, GI tolerance, metabolic markers, hydration, body composition, and access reality. |
- Retatrutide belongs in a trial-readiness conversation, not a retail protocol conversation.
- Eligibility, exclusions, monitoring, and adverse-event capture are part of the intervention context.
- Escalation in trials is protocol-defined and supervised.
- The Blueprint should not turn those study arms into dosing advice.
- Clinical trials evaluate weight, adverse effects, metabolic markers, and discontinuation patterns over many months.
- Early appetite change should not be treated as proof of long-term fit.
- No approved maintenance label exists for this dossier.
- Long-term maintenance, access, and post-approval labeling remain unsettled.
- The practical decision is whether to wait for regulated evidence and access, not how to self-assemble a protocol.
- Research-only sourcing changes the risk profile materially.
| Item | Reference |
|---|---|
| Reference framing | Clinical-trial weekly subcutaneous escalation |
| Frequency | Once weekly in study designs |
| Route | Subcutaneous |
| Decision points | Trial eligibility, tolerability, metabolic markers, hydration, and body composition |
| Current use context | Research and clinical-trial framing, not routine consumer access |
- Is the user reading trial data as evidence context or as a do-it-yourself protocol?
- Is the compound available through a legitimate trial or only through research-only channels?
- Is the user treating an unapproved or compounded retatrutide source as lawful or equivalent to trial supply?
- Are GI symptoms, hydration, nutrition, glucose markers, and body composition being monitored?
- Is the user comparing retatrutide against approved options with clearer labels?
- Is the access path itself the main safety issue?
- Trial dose groups, escalation rules, and duration by study protocol.
- Eligibility criteria by trial population and indication.
- Evidence maturity as phase 3 data and regulatory review evolve.
- How strongly a future label may differ from the phase 2 design.
- Treating investigational trial exposure as an approved label.
- Assuming research-only retatrutide is equivalent to clinical-trial drug supply.
- Assuming retatrutide can be compounded or sourced like an approved GLP-1 medication.
- Combining with other incretin or appetite-active compounds outside professional review.
- Ignoring adverse effects because the compound is described as next-generation.
- Using community vial conversions as if they were study protocol.
Administration details for retatrutide should remain tied to trial protocol and regulated study supply. The Blueprint does not provide injection instructions for research-only products.
- Read once-weekly trial exposure as study context, not access guidance.
- Do not infer vial concentration, storage, reconstitution, or syringe units from trial publications.
- Use research-only or compounded retatrutide claims as a regulatory and quality risk flag, not a shortcut around clinical oversight.
Retatrutide does not have a settled maintenance label in this dossier. Maintenance should be framed as an unanswered regulatory and evidence question.
- Wait for phase 3, labeling, and post-approval guidance before treating maintenance as knowable.
- Compare against approved incretins when the user needs an actionable current path.
- Do not use plateau or regain concerns as a reason to self-combine investigational compounds.
| Question | Reference answer |
|---|---|
| Is there an approved retatrutide protocol? | No approved consumer label is used in this Blueprint. The reference is clinical-trial context. |
| How often was it studied? | Published obesity research used once-weekly subcutaneous exposure in trial settings. |
| Can trial doses be copied? | No. Trial dose groups are study design, not individualized instructions. |
| What is the main practical blocker? | Regulatory maturity and access quality, not just mechanism. |
| What should be compared first? | Approved options with clearer labels and monitoring paths remain the practical comparison set. |
Educational reference only. Retatrutide is investigational in this context and this is not a prescription or access recommendation.
- Do not treat pipeline access as equivalent to approved medication.
- Do not stack with other incretin agents outside professional review.
- Do not ignore GI symptoms, dehydration, or rapid intake collapse.
- Do not use trial-stage status as a reason to bypass clinical oversight.
Monitoring and labs
- Weight and waist circumference
- Body composition if available
- Fasting glucose and HbA1c
- Liver and kidney function
- Medication review
- Contraindication history
- GI tolerance
- Hydration
- Protein intake
- Energy and training continuity
- Glucose response
- Symptoms that persist or intensify
- Lean mass
- Plateau pattern
- Metabolic labs
- Access and study-status updates
- Maintenance strategy
Monitoring should reflect both the incretin-like side-effect pattern and the extra uncertainty of a pipeline-stage compound.
Regulatory status & study stage
Retatrutide is an investigational triple agonist. It is clinically important, but it is not an FDA-approved weight-management medication.
| Item | Status | How to read it |
|---|---|---|
| Retatrutide | Phase 3 / investigational | A promising clinical-trial compound, not an approved medication pathway. |
| Mechanism category | GLP-1 / GIP / glucagon triple agonist | A next-generation incretin approach with a higher theoretical ceiling. |
| Access | Clinical-trial or research framing | Not equivalent to branded prescription access for approved drugs. |
- Strong Phase 2 signal with Phase 3 development context.
- Not yet mature post-market evidence.
- Approval, label, and access remain future-dependent.
- No routine FDA-approved prescription pathway for weight management.
- Trial access is different from consumer access.
- Compounded retatrutide should not be treated as a lawful substitute for trial or approved supply.
- Research-only products should not be treated as equivalent to legitimate clinical development.
Pipeline status is not a technicality. It changes evidence maturity, access, liability, and practical fit.
Stacking and synergies
For retatrutide, stacking should be read even more conservatively because the compound itself already targets multiple pathways.
- Retatrutide plus protein and resistance training strategy in trial-style framing.
- Retatrutide plus careful body-composition monitoring.
- Retatrutide plus hydration and GI-tolerance tracking.
- Retatrutide plus semaglutide, tirzepatide, or another incretin without professional review.
- Retatrutide plus another strong appetite suppressant.
- Glucose-lowering medication
- Insulin
- Other incretins
- Aggressive weight-loss protocols
- Any research-only sourcing scenario
Do not combine multi-agonist incretin pathways casually; redundancy can increase risk without making the signal easier to understand.
Genetic variable
Genetic context may eventually matter for GLP-1, GIP, glucagon, appetite, and insulin-response pathways, but retatrutide-specific pharmacogenomics remain early.
- Metabolic and appetite genetics can inform background risk.
- GLP-1/GIP/glucagon pathway genes may become useful expectation modifiers.
- No SNP should be used to claim a retatrutide response pattern today.
Genetics should be treated as an expectation layer, not a reason to bypass evidence maturity.
Real-world reports
- High interest due to weight-loss ceiling
- GI concerns similar to the incretin category
- Curiosity from prior GLP-1 users
- Confusion between trial data and access reality
- Speculation around future superiority
- Not approved
- Access uncertainty
- GI tolerance concern
- Research-only quality risk
- Preference for approved pathways
- Most real-world discussion is expectation-setting, not mature clinical use.
- Pipeline enthusiasm should be separated from current practical fit.
- Anecdotes cannot substitute for approval and long-term evidence.
Final personalized interpretation
For Ana, retatrutide is interesting because the profile suggests more than a light appetite-control need. PCOS, metformin use, food-noise pressure, prior semaglutide exposure, and a significant weight-loss objective all make high-ceiling incretin biology relevant.
The reason it sits below tirzepatide and semaglutide is not mechanism. It is maturity. Ana's Blueprint should privilege options that combine fit with practical access, evidence maturity, and a clear monitoring path.
If Ana's prior GLP-1 experience created a plateau, retatrutide is the type of compound that explains where the field is moving. But pipeline relevance is not the same as a current recommendation, especially when preserving lean mass and tolerability are already central concerns.
The best interpretation is that retatrutide belongs in the watchlist tier: scientifically relevant, potentially powerful, but not the first practical conversation compared with approved incretin options.
The Match Score reflects future-facing relevance. The decision weight should still favor maturity, access, safety review, and the ability to monitor the intervention responsibly.