PTD-DBM
A Wnt-pathway hair research compound with very low readiness.
PTD-DBM is framed in Hair Loss as wnt / beta-catenin / cxxc5 pathway research. The dossier separates mechanism, human outcome evidence, regulatory status, and Ana-specific fit.
PTD-DBM belongs in this niche because it helps explain high-interest wnt hair-regrowth research boundary. The report keeps the interpretation educational, source-bound, and non-prescriptive.
Why it may make sense for you
Ana's thinning makes the research narrative visible, but it is not a practical candidate.
| Signal | Interpretation |
|---|---|
| Profile driver | Ana's thinning makes the research narrative visible, but it is not a practical candidate. |
| Main caution | Growth-pathway modulation and preclinical status require strong caution. |
| Evidence read | Preclinical and early translational; not ready as consumer hair therapy. |
| Practical read | Very low; included to explain advanced research claims. |
- Explains a highly searched hair-regrowth research pathway.
- Mechanistically relevant to follicle cycling.
- Useful as a boundary marker.
- Preclinical readiness.
- Growth-signaling caution.
- No practical consumer protocol.
How it works
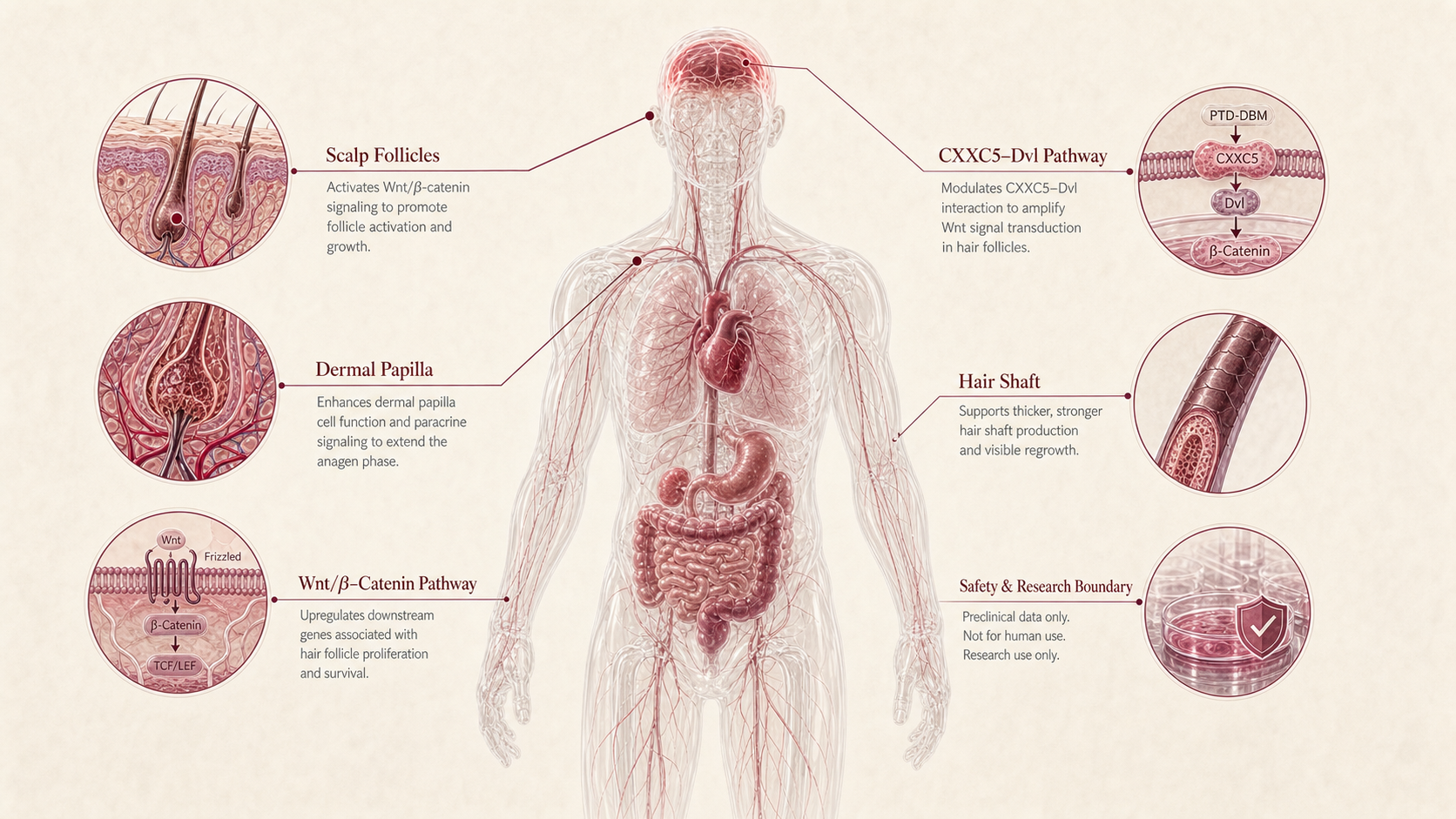
PTD-DBM is discussed around disrupting CXXC5-Dvl interaction to modulate Wnt/beta-catenin follicle signaling in hair-growth research.
| Pathway | Practical effect |
|---|---|
| Mechanism family | Wnt / beta-catenin / CXXC5 pathway research. |
| Target context | PTD-DBM Wnt/beta-catenin hair-regeneration research literature. |
| Safety boundary | Wnt/beta-catenin growth signaling is not casual cosmetic territory. |
PTD-DBM is useful to understand one pathway in Hair Loss; it is not a complete plan and should not override the foundation.
What the evidence shows
PTD-DBM has three evidence layers in this report: mechanism, human or cosmetic outcome evidence, and regulatory/readiness evidence. Peptivius keeps those layers separate so market interest does not become a treatment claim.
| Study | Population | Key result | How to read it |
|---|---|---|---|
| Mechanism | Wnt / beta-catenin / CXXC5 pathway research. | PTD-DBM is discussed around disrupting CXXC5-Dvl interaction to modulate Wnt/beta-catenin follicle signaling in hair-growth research. | Pathway plausibility. |
| Human / applied evidence | Human practical evidence remains insufficient for consumer recommendation. | Preclinical and early translational; not ready as consumer hair therapy. | Outcome translation. |
| Regulatory / access | No approved hair-loss label; preclinical/research context. | Very low; included to explain advanced research claims. | Readiness boundary. |
- User-specific response is not validated by this report.
- Route, formulation, identity, and jurisdiction can change the interpretation.
- Combination evidence is not assumed from individual-compound evidence.
Safety, side effects, and contraindications
- Evidence and safety depend on route, formulation, product identity, and clinical context.
- Research-only and cosmetic-context products should not be treated as approved therapeutic products.
- Side effects, contraindications, and monitoring requirements can differ from market summaries.
- Preclinical readiness.
- Growth-signaling caution.
- No practical consumer protocol.
- Pregnancy, fertility treatment, breastfeeding, active malignancy or cancer history, autoimmune activity, endocrine disease, and major psychiatric or cardiovascular context require professional review when relevant.
- Medication context matters for Ana, especially levothyroxine, escitalopram, metformin, PCOS, Hashimoto, and sleep limitations.
- Do not combine mechanisms, routes, or products without clinical oversight.
Growth-pathway modulation and preclinical status require strong caution.
Reference protocol
Preclinical Wnt hair-regrowth boundary: PTD-DBM is anchored to PTD-DBM Wnt/beta-catenin hair-regeneration research literature. inside the Hair Loss niche. This is reference literacy, not a personal protocol.
- Hair Loss marketing claims without source-quality review.
- Research-only, compounded, grey-market, or cosmetic-context products treated as approved therapeutic products.
- Community protocols, dose charts, vial math, supplier claims, or stack templates.
| Item | Reference |
|---|---|
| Reference context | Preclinical Wnt hair-regrowth boundary |
| Route literacy | Topical |
| Application footprint | Context-specific; no operational protocol is provided. |
| Escalation style | Not defined by Peptivius; clinical or product context controls interpretation. |
| Main checkpoints | Wnt/beta-catenin growth signaling is not casual cosmetic territory. |
- Confirm whether the claim is label-based, trial-based, cosmetic, regional-use, preclinical, or research-sensitive.
- Separate the peptide identity from products, blends, salts, marketing names, or route changes.
- Ana's thinning makes the research narrative visible, but it is not a practical candidate.
- Read the compound against Ana's declared goals, conditions, medications, and safety constraints.
- Growth-pathway modulation and preclinical status require strong caution.
- Do not turn this reference into dosing, sourcing, stacking, timing, cycling, or treatment instructions.
| Item | Reference |
|---|---|
| Reference mode | Preclinical Wnt hair-regrowth boundary |
| Primary anchor | PTD-DBM Wnt/beta-catenin hair-regeneration research literature. |
| Route | Topical |
| Main checkpoint | Wnt/beta-catenin growth signaling is not casual cosmetic territory. |
- Is the Hair Loss concern better explained by sleep, stress, thyroid, PCOS, nutrition, medication, diagnosis, training load, or routine before a peptide is considered?
- Is the evidence human outcome evidence, mechanistic evidence, cosmetic evidence, label evidence, or market narrative?
- Does Ana's Hashimoto, PCOS, SSRI use, metformin use, sleep limitation, or injury context change the professional-review threshold?
- Would adding this compound reduce attribution clarity or overlap with another mechanism already ranked in the Blueprint?
- Jurisdiction, formulation, route, product identity, and clinical setting.
- Whether the claim is cosmetic, investigational, label-adjacent, or purely mechanistic.
- How strongly the compound belongs in this niche versus a neighboring niche.
- Regulatory status and indication boundaries.
- Contraindications, medication interactions, pregnancy/fertility context, autoimmune context, and product identity.
- Route changes, injectable versus topical assumptions, and claims borrowed from unrelated evidence.
Administration details are included only as route literacy. Peptivius does not publish instructions for obtaining, preparing, mixing, injecting, applying, or escalating peptides.
- Approved-product labels, clinical trials, topical cosmetic use, and research-only discussion are separate contexts.
- Route and formulation can change both safety and interpretation.
- Any operational plan belongs with a licensed professional or the product's regulated instructions where applicable.
Maintenance means tracking whether the original problem is improving and whether the evidence boundary still makes sense.
- Reassess the underlying driver rather than layering more mechanisms.
- Pause interpretation when sleep, stress, nutrition, thyroid, PCOS, medication, diagnosis, or recovery load changes.
- Avoid stack escalation when benefit, side effects, or source quality cannot be attributed cleanly.
| Question | Reference answer |
|---|---|
| Is this a protocol? | No. This block is context for reading the peptide, not a dosing or use plan. |
| Can this replace medical care? | No. Diagnosis, medication review, labs, and clinician review remain separate from peptide education. |
| Why include lower-evidence compounds? | Because highly searched compounds deserve evidence boundaries when users encounter them. |
PTD-DBM has no Peptivius protocol in this Blueprint. The reference block is limited to evidence boundaries, source quality, and decision checkpoints.
- Do not convert this into dosing, timing, vial, syringe, cycling, sourcing, or stack guidance.
- Do not treat research-only, cosmetic, or regional-use evidence as an approved indication.
- Do not layer with neighboring niche mechanisms just because the names appear together online.
Monitoring and labs
- Clarify the actual problem pattern, severity, duration, triggers, current routine, medications, labs when relevant, and red flags.
- Separate cosmetic, performance, endocrine, neurological, sexual, or dermatologic goals from medical diagnosis.
- Track the target outcome, adverse effects, attribution, and changes in sleep, stress, nutrition, training, medications, and symptoms.
- Reassess whether the foundation explains more than the peptide narrative.
- Keep the primary foundation visible: diagnosis, sleep, nutrition, training, stress, endocrine review, dermatology/sexual-health care, or medication review as applicable.
- Avoid escalation when causality is unclear.
Monitoring is outcome and safety literacy, not a protocol tracker.
Regulatory status & study stage
No approved hair-loss label; preclinical/research context.
| Item | Status | How to read it |
|---|---|---|
| Status | Preclinical | Read only inside the stated anchor. |
| Niche role | High-interest Wnt hair-regrowth research boundary. | Hair Loss |
| Evidence maturity | Preclinical and early translational; not ready as consumer hair therapy. | Mechanism, outcome, and regulatory status remain separate. |
- Human practical evidence remains insufficient for consumer recommendation.
- Market visibility is not equivalent to clinical readiness.
- Very low; included to explain advanced research claims.
- No supplier, price, preparation, or dosing pathway is provided.
This dossier does not translate static category education into a personal use plan.
Stacking and synergies
PTD-DBM may appear in Hair Loss stack discussions online, but Peptivius keeps combination literacy at the niche level. This dossier evaluates the individual compound.
- Foundation work, diagnostic clarity, sleep, nutrition, stress reduction, medication review, and condition-specific care.
- Professional review when endocrine, psychiatric, autoimmune, cardiovascular, fertility, dermatologic, or sexual-health context is present.
- Objective tracking of the problem pattern before and after any major change.
- Multiple compounds with overlapping mechanisms used to chase a broad outcome.
- Cosmetic, research-only, and approved-drug contexts blended as if they carry the same safety profile.
- Adding peptides when the limiting driver is sleep, stress, nutrition, medication, diagnosis, or training load.
- Pregnancy, fertility treatment, breastfeeding, cancer history, autoimmune disease, endocrine disease, psychiatric medication, cardiovascular risk, severe symptoms, or unclear diagnosis.
- Any attempt to combine this compound with another peptide, hormone-active drug, sexual-health drug, or cosmetic procedure.
More mechanisms do not automatically mean a better result. Layering compounds can reduce attribution and increase monitoring burden.
Genetic variable
PTD-DBM has no validated consumer genetic response engine in Peptivius today. The genes below are pathway literacy only.
- No validated consumer genotype determines response for this dossier.
- Pathway genes may help explain why the topic matters biologically.
- No SNP should convert this peptide into a treatment recommendation.
Future DNA layers may improve interpretation, but Slice 1 does not personalize this dossier from genotype.
Real-world reports
- PTD-DBM appears in user discussions around high-interest wnt hair-regrowth research boundary.
- Reports often mix peptides with supplements, procedures, medication changes, lifestyle changes, and other compounds.
- Market popularity can reveal what users search for, but does not prove efficacy.
- No meaningful change in the target outcome.
- Adverse effects, unclear attribution, worsening symptoms, or new red flags.
- Concern that experimentation is delaying diagnosis or standard care.
- Anecdotes are discovery signals, not clinical proof.
- Benefit and side effect attribution are weak when several changes happen at once.
- The safest read is source-bound, conservative, and anchored to the niche foundation.
Final personalized interpretation
For Ana, PTD-DBM is interpreted against hair loss is active because ana reported ludwig ii thinning, pcos context, ferritin deficiency, hashimoto, stress, poor sleep, and recent restrictive dieting.
Ana's thinning makes the research narrative visible, but it is not a practical candidate. Growth-pathway modulation and preclinical status require strong caution.
The practical conclusion is conservative: PTD-DBM is a Hair Loss education and professional-conversation topic, not a use instruction.
Important research narrative, but not ready for practical use. Peptivius keeps this as interpretation, not a protocol.