LL-37
Antimicrobial host-defense peptide for SIBO and dysbiosis literacy, not a broad microbiome protocol.
LL-37 in Gut Health is framed as antimicrobial host-defense peptide / innate immune and barrier context. The report separates mechanism, human gut-health outcome evidence, and regulatory status.
LL-37 helps explain sibo, dysbiosis, antimicrobial peptide, and host-defense literacy. For Ana, it is evaluated against bloating, food triggers, suspected permeability, anxiety-linked gut unpredictability, Hashimoto, PCOS, metformin use, and lack of a confirmed IBD/SIBO diagnosis.
Why it may make sense for you
For Ana, LL-37 appears because the Gut Health profile combines persistent bloating, multiple food triggers, suspected permeability, anxiety around intestinal unpredictability, Hashimoto, PCOS, metformin use, and no robust formal GI diagnosis.
| Signal | Interpretation |
|---|---|
| Primary symptom pattern | Constant bloating and food-triggered symptoms |
| Barrier question | Suspected leaky gut / permeability |
| Inflammatory context | Hashimoto, PCOS, low-grade inflammation |
| Gut-brain context | Anxiety linked to intestinal unpredictability |
| Diagnostic boundary | No confirmed IBD, SIBO, celiac disease, or short bowel syndrome |
- Ana reports multiple food triggers and suspected dysbiosis/SIBO-like concerns without a confirmed diagnosis.
- The dossier helps separate barrier, inflammation, motility, dysbiosis, and regulated GLP-2 categories.
- Ana has enough gut-context signals for education to be useful.
- Without diagnostic confirmation, antimicrobial logic can cause more confusion than clarity.
- Food triggers and bloating can reflect intolerance, celiac disease, IBS, SIBO, medication effects, reflux, thyroid context, or inflammatory disease.
- Red flags should move the conversation to medical evaluation, not peptide matching.
How it works
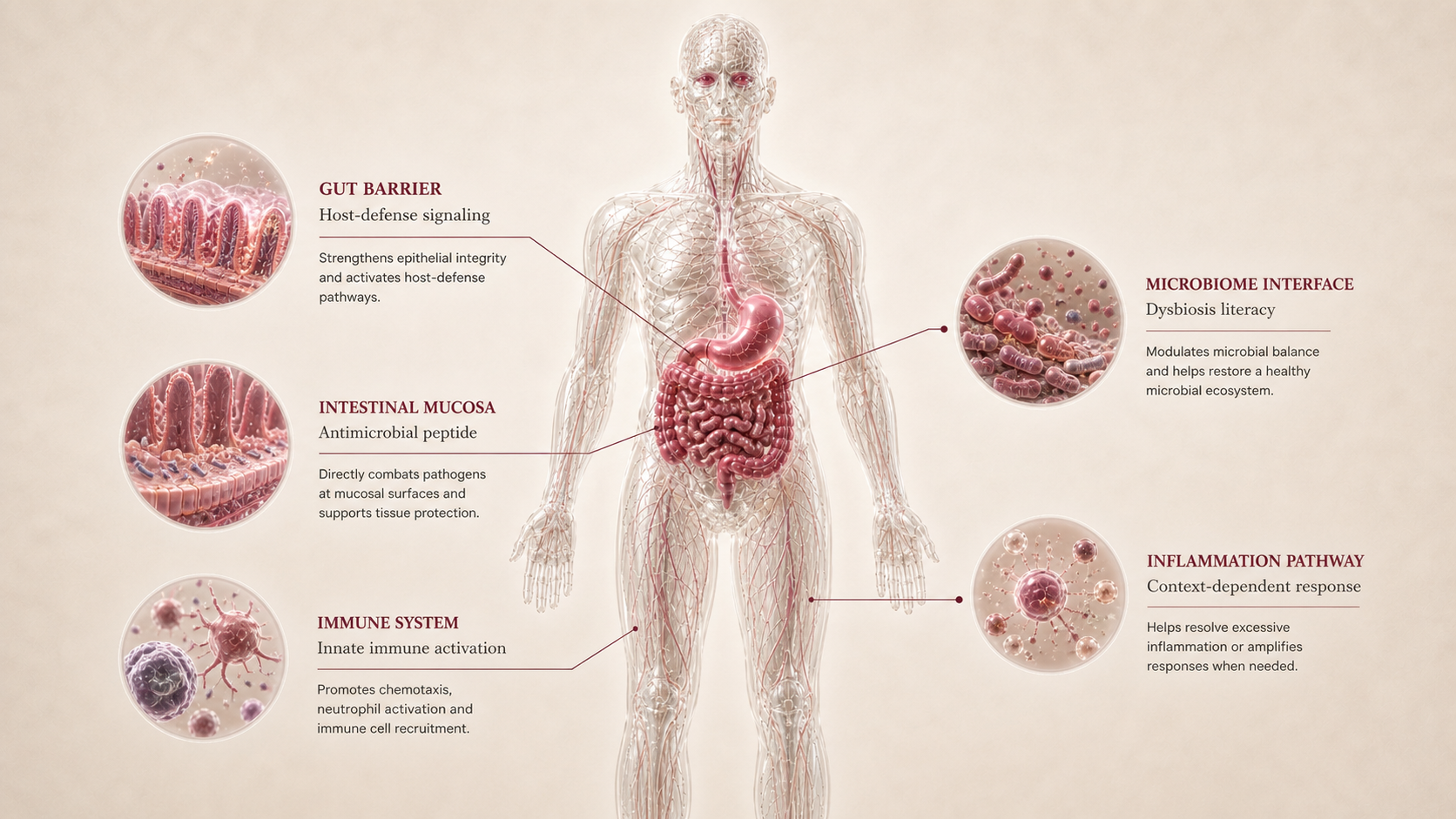
LL-37 is a human cathelicidin-derived antimicrobial peptide involved in host defense, epithelial barrier signaling, immune modulation, microbial interaction, and inflammation. That makes it relevant to dysbiosis literacy but also harder to simplify safely.
| Pathway | Practical effect |
|---|---|
| Mechanistic evidence | Antimicrobial host-defense peptide / innate immune and barrier context. |
| Human gut-health outcome evidence | Human gut-health outcomes remain early and indirect; mechanistic host-defense biology does not prove SIBO treatment efficacy. |
| Regulatory / label evidence | FDA safety-risk materials state that safety information is insufficient to know whether cathelicidin LL-37 would cause harm when administered to humans. |
| Ana relevance | SIBO, dysbiosis, antimicrobial peptide, and host-defense literacy. |
LL-37 is useful for understanding one gut pathway, but a pathway is not the same as diagnosis, treatment, or a protocol.
What the evidence shows
LL-37 is framed through three evidence layers: mechanism, human gut-health outcomes, and regulatory/label status. Peptivius keeps these separate so gut-health marketing does not turn a plausible pathway into a treatment claim.
| Study | Population | Key result | How to read it |
|---|---|---|---|
| Mechanistic evidence | Antimicrobial host-defense peptide / innate immune and barrier context. | LL-37 is a human cathelicidin-derived antimicrobial peptide involved in host defense, epithelial barrier signaling, immune modulation, microbial interaction, and inflammation. That makes it relevant to dysbiosis literacy but also harder to simplify safely. | Explains why the peptide appears in Gut Health discussions. |
| Human gut-health outcome evidence | Outcome translation | Human gut-health outcomes remain early and indirect; mechanistic host-defense biology does not prove SIBO treatment efficacy. | Determines how far the claim can go. |
| Regulatory / label evidence | Research Only | FDA safety-risk materials state that safety information is insufficient to know whether cathelicidin LL-37 would cause harm when administered to humans. | Defines practical boundary and approved-context status. |
- Whether the user's symptoms are IBS, IBD, SIBO, reflux, intolerance, celiac disease, medication-related, thyroid-linked, or another pattern.
- Whether human evidence supports the same claim being discussed in forums.
- Whether product identity, route, formulation, or source quality changes the risk profile.
Safety, side effects, and contraindications
- Gut symptom attribution can be unclear.
- Route/formulation uncertainty can change interpretation.
- Placebo, diet changes, and co-interventions can dominate perceived effects.
- SIBO/dysbiosis claims are easy to overread; antimicrobial and inflammatory effects are context-dependent.
- Blood in stool, anemia, fever, nocturnal diarrhea, progressive pain, persistent vomiting, dysphagia, dehydration, or unintentional weight loss require evaluation.
- Active IBD, suspected infection, immunosuppression, chronic corticosteroid use, pregnancy, or cancer history need professional review.
- Research-only, compounded, and grey-market products are not equivalent to approved gut medications.
- Red-flag GI symptoms without evaluation.
- Known or suspected obstruction, severe dehydration, acute abdomen, or rapidly worsening abdominal pain.
- Active serious infection or uncontrolled inflammatory disease without clinician oversight.
- Pregnancy or lactation without medical supervision.
- Using a peptide to delay diagnosis or standard care.
For Ana, LL-37 should be read through the fact that symptoms are persistent but not yet diagnostically settled. The priority is pattern clarity, food-trigger mapping, labs/testing when appropriate, and red-flag screening.
Reference protocol
Research-sensitive mechanism context: FDA safety-risk context for cathelicidin LL-37 plus LL-37 inflammatory bowel disease and antimicrobial peptide literature.
- Diagnosis, medical evaluation, endoscopy, stool testing, breath testing, celiac workup, or gastroenterology care.
- A personal protocol, dose plan, stack, supplier path, or treatment recommendation.
- Community protocols, compounded blends, or research-only products marketed as gut-healing solutions.
| Item | Reference |
|---|---|
| Reference frame | Research-only antimicrobial peptide context |
| Gut role | SIBO, dysbiosis, antimicrobial peptide, and host-defense literacy. |
| Evidence layer | Mechanistic and early gut/IBD-host-defense interest; limited direct human gut-health outcome evidence. |
| Practical readiness | Low; research-only antimicrobial peptide context, not a consumer microbiome protocol. |
| Not a protocol | No dose, timing, cycle, vial, syringe, unit, or supplier guidance. |
- Clarify the symptom pattern, food triggers, medication context, prior workup, and red flags.
- Separate barrier, inflammation, motility, reflux, dysbiosis, celiac, and malabsorption hypotheses.
- Use professional review when symptoms are severe, progressive, inflammatory, or unexplained.
- Read LL-37 as research-only antimicrobial peptide context, not as a consumer use plan.
- Keep mechanism, human outcome evidence, and regulatory status separated.
- Avoid treating gut discomfort as one universal category.
- Track symptoms, stool pattern, food tolerance, reflux, energy, weight change, hydration, and new red flags.
- Escalate evaluation rather than peptide experimentation when alarm features appear.
- Treat stopping, deferring, or seeking workup as a valid conclusion.
| Item | Reference |
|---|---|
| Reference mode | Research-only antimicrobial peptide context |
| Primary anchor | FDA safety-risk context for cathelicidin LL-37 plus LL-37 inflammatory bowel disease and antimicrobial peptide literature. |
| Route label | Subcutaneous as category descriptor, not instruction. |
| Timing | No consumer protocol timeline. |
| Decision points | Diagnosis, red flags, food triggers, medications, labs/testing, and professional review. |
- Is this barrier, inflammation, motility, reflux, dysbiosis, celiac, or malabsorption?
- Are red flags present?
- Has a clinician ruled out conditions that should not be self-managed?
- Would a peptide obscure the diagnosis or reduce clarity?
- Is the evidence layer being confused with a treatment plan?
- Which gut hypothesis is most relevant.
- Which tests or clinical review are needed.
- How food triggers, stress, medication, and thyroid/metabolic context change the interpretation.
- Red-flag triage.
- Approved indication boundaries.
- The difference between research-only peptides and approved medications.
- Avoidance of dose conversions, cycles, blends, and supplier guidance.
Administration is included only as category literacy. The report does not instruct the reader to administer a gut peptide.
- Route labels in the report are descriptive, not recommendations.
- Gut peptides are especially easy to over-market because symptoms are common and nonspecific.
- Product identity, route, formulation, and source quality can dominate safety interpretation.
Gut Health maintenance is about diagnostic clarity, symptom stability, sustainable diet, and professional care when needed.
- Track food tolerance and symptom patterns rather than chasing a peptide timeline.
- Revisit labs, stool markers, or gastroenterology evaluation if symptoms persist.
- Do not use peptides to delay care for inflammatory, bleeding, obstructive, or malabsorptive patterns.
| Question | Reference answer |
|---|---|
| Is this a gut protocol? | No. It is mechanism and evidence literacy. |
| Can this replace a gastroenterologist? | No. Diagnosis and red-flag evaluation come first. |
| Can I treat SIBO, IBD, or leaky gut with this? | The report does not make that recommendation. |
| Why include regulatory anchors? | They show what approved gut peptide evidence looks like, and where the boundaries are. |
Reference context only. This dossier does not provide a dose, schedule, duration, cycle, vial conversion, syringe unit, supplier path, or personal protocol.
- Do not treat gut discomfort as one universal peptide problem.
- Do not use peptide matching to delay evaluation of red flags.
- Do not infer a stack, blend, or protocol from mechanism overlap.
- Do not treat research-only products as equivalent to approved medications.
Monitoring and labs
- Bowel pattern, stool frequency, urgency, constipation, diarrhea, and nocturnal symptoms.
- Pain, bloating, reflux, nausea, vomiting, hydration, and weight trend.
- Food triggers: gluten, lactose, FODMAPs, meal timing, alcohol, caffeine, and supplements.
- Medication context: metformin tolerance, thyroid medication, acid suppression, NSAIDs, antibiotics, and probiotics.
- Prior workup: celiac testing, stool tests, SIBO breath testing, endoscopy history, fecal calprotectin if applicable.
- CBC, ferritin, B12, vitamin D, inflammatory markers, and thyroid/metabolic context when relevant.
- Symptom frequency and intensity.
- Food tolerance and trigger consistency.
- Diarrhea, constipation, reflux, pain at night, hydration, energy, and weight.
- New red flags or symptom progression.
- Whether a structured diet or clinical evaluation has clarified the pattern.
- Stable symptom pattern and known triggers.
- Sustainable diet strategy rather than endless restriction.
- Need for gastroenterology follow-up or further testing.
- Response to conventional care when indicated.
- Relationship with sleep, stress, anxiety, and gut-brain patterns.
The goal is not just reducing discomfort. It is understanding the pattern, identifying red flags, avoiding overclaiming, and building a safe strategy.
Regulatory status & study stage
FDA safety-risk materials state that safety information is insufficient to know whether cathelicidin LL-37 would cause harm when administered to humans.
| Item | Status | How to read it |
|---|---|---|
| Status | Research Only | Interpret only inside the stated anchor. |
| Gut indication | SIBO, dysbiosis, antimicrobial peptide, and host-defense literacy. | Not all gut roles are clinical indications. |
| Readiness | Low; research-only antimicrobial peptide context, not a consumer microbiome protocol. | Practical readiness is separate from mechanism interest. |
- Human gut-health outcomes remain early and indirect; mechanistic host-defense biology does not prove SIBO treatment efficacy.
- Gut symptoms require diagnostic context before outcome claims can be interpreted.
- Low; research-only antimicrobial peptide context, not a consumer microbiome protocol.
- No supplier, dose, or protocol guidance is provided.
This dossier does not convert label, trial, research, or comparator context into consumer instructions.
Stacking and synergies
LL-37 may appear in gut-healing stacks online, but Peptivius keeps combination literacy at the niche level. This dossier evaluates the individual peptide.
- Symptom journal, food-trigger mapping, hydration, and bowel-pattern tracking.
- Clinician-guided testing when celiac disease, IBD, SIBO, malabsorption, or reflux complications are possible.
- Sleep and stress support when gut-brain patterns are present.
- Multiple gut peptides layered without a diagnosis.
- Barrier plus antimicrobial plus immune peptides used as a broad gut-healing blend.
- Adding peptides while ignoring metformin tolerance, thyroid context, or dietary triggers.
- Blood, anemia, weight loss, nocturnal diarrhea, severe pain, vomiting, or dysphagia.
- Known IBD, celiac disease, immunosuppression, chronic steroid use, or suspected infection.
- Any antimicrobial peptide or GLP-2 class discussion.
A gut stack can reduce clarity. If symptoms change, it becomes harder to know whether food, medication, infection, inflammation, placebo, or a peptide caused the change.
Genetic variable
LL-37 has no validated consumer genetic response engine in Peptivius today. The genes below are pathway literacy only for barrier, immune, motility, celiac, or microbiome-related interpretation.
- No validated genotype determines whether this peptide is appropriate for Ana.
- Pathway genes may help explain barrier, immune, motility, or celiac-risk differences.
- No SNP should convert gut symptoms into a peptide recommendation.
Future DNA layers may refine gut interpretation, but Slice 1 does not personalize gut peptides from genotype.
Real-world reports
- Gut-health anecdotes often mix peptides with elimination diets, probiotics, antibiotics, supplements, and stress changes.
- Users frequently report nonspecific symptoms such as bloating, reflux, constipation, or food reactivity without a confirmed diagnosis.
- Research-only product quality and route claims are recurring concerns.
- New red flags or symptom progression.
- Unclear diagnosis or worsening GI symptoms.
- Concern that a peptide is masking the need for standard evaluation.
- Anecdotes can reveal what users ask, but they do not prove gut-health efficacy.
- The strongest interpretation comes from diagnosis, symptom tracking, labs/testing, and response to conventional foundations.
- Blend marketing should be decomposed into component mechanisms.
Final personalized interpretation
For Ana, LL-37 is best read through a diagnostic-clarity lens. The profile has meaningful gut signals: persistent bloating, suspected permeability, gluten/lactose/FODMAP triggers, anxiety around unpredictability, Hashimoto, PCOS, metformin exposure, and low-grade inflammatory context.
That does not mean the problem is automatically leaky gut, SIBO, IBD, or reflux. It means the report should separate barrier, inflammation, gut-brain, motility, dysbiosis, celiac/permeability, and regulated GLP-2 concepts before any peptide receives too much credit.
LL-37 is useful because it explains one part of that map. It does not replace gastroenterology review, red-flag triage, stool/lab testing when appropriate, structured diet work, or medication review.
For Ana, LL-37 should be read as Gut Health education, not a protocol or treatment instruction.