Liraglutide
An older GLP-1 option with established evidence, daily dosing, and a lower practical ceiling than newer weekly agents.
GLP-1 receptor agonist administered by daily subcutaneous injection in approved diabetes and chronic weight-management indications.
Liraglutide works through the same broad GLP-1 appetite and glucose pathway as semaglutide, but with daily administration and generally less compelling practical fit in a modern Weight Loss ranking.
Why it may make sense for you
For Ana, liraglutide appears as a secondary GLP-1 option. It fits the appetite and metabolic category, but daily dosing and lower practical ceiling make it less attractive than semaglutide or tirzepatide.
| Signal | Interpretation |
|---|---|
| Declared objective | Weight loss and recomposition |
| Mechanism fit | GLP-1 appetite and glucose pathway |
| Practical limitation | Daily injection burden |
| Category role | Fallback or comparator rather than lead option |
| Rank reason | Lower ceiling and adherence friction |
- Clinically familiar GLP-1 mechanism.
- Can support appetite and satiety goals.
- May matter when weekly agents are not accessible.
- Established enough to compare against newer options.
- Daily administration is less aligned with Ana's need for sustainable adherence.
- May be less compelling after prior semaglutide exposure.
- GI tolerance and nutrition regularity still require monitoring.
- Not the highest-fit option for significant weight-loss objectives.
How it works
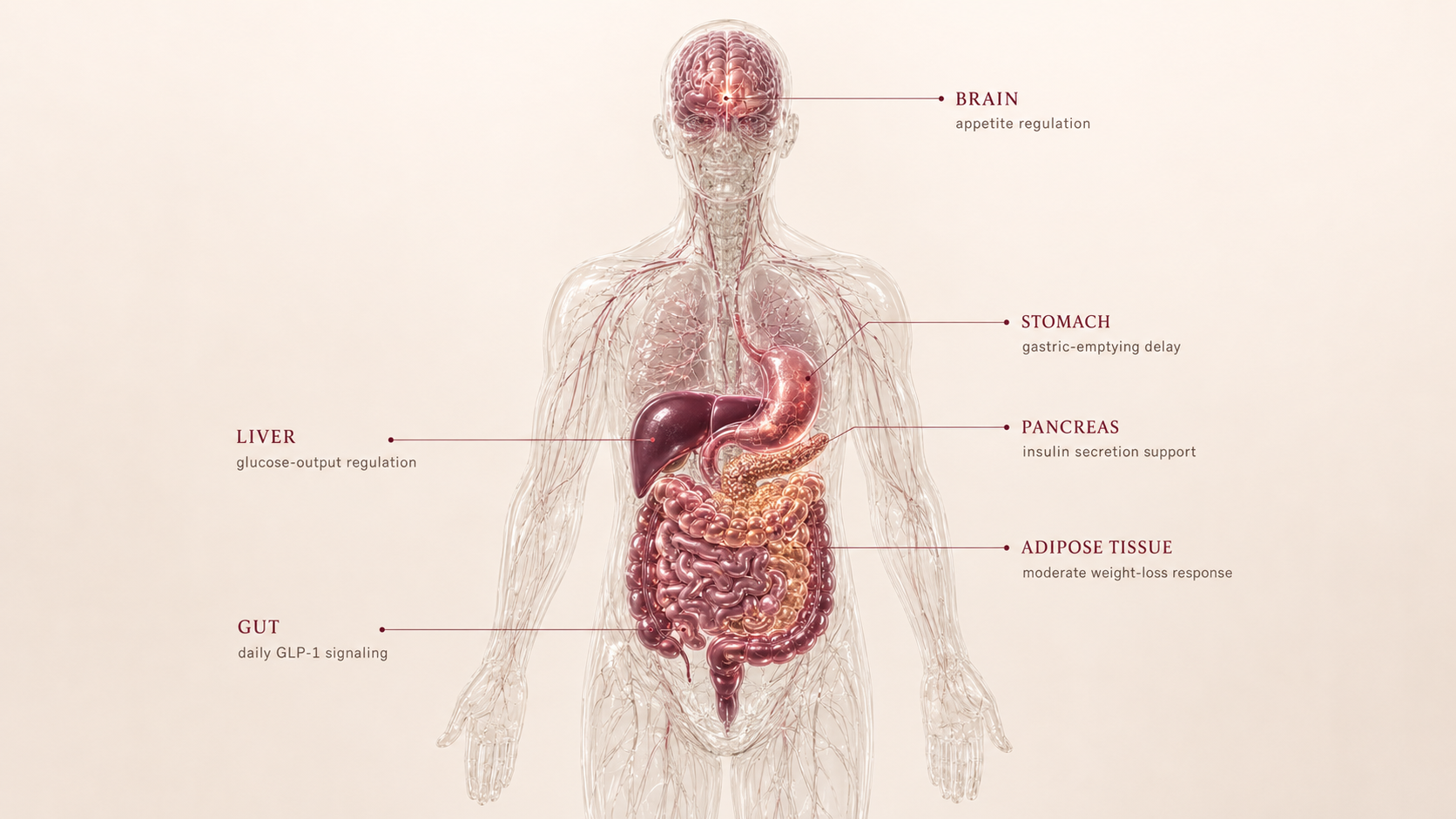
Liraglutide activates GLP-1 receptors, helping increase satiety, slow gastric emptying, and improve glucose-dependent insulin response. The mechanism is familiar; the main difference is daily exposure rather than a weekly formulation.
| Pathway | Practical effect |
|---|---|
| GLP-1 receptor | Satiety and appetite reduction |
| Stomach | Slower gastric emptying |
| Pancreas | Glucose-dependent insulin support |
| Routine | Daily injection creates adherence load |
Liraglutide is a daily GLP-1: useful biology, but less convenient and usually less compelling than newer weekly options.
What the evidence shows
Liraglutide has established evidence in diabetes and weight-management contexts, but its position in the modern category is often as an older comparator rather than the highest-ceiling option.
| Study | Population | Key result | How to read it |
|---|---|---|---|
| SCALE weight-management program | Adults with obesity or overweight | Clinically relevant weight-loss signal | Supports liraglutide as an established GLP-1 weight-management option |
| Diabetes clinical programs | People with type 2 diabetes | Glycemic improvement with weight effects | Relevant for metabolic-risk profiles |
| Modern category comparison | GLP-1/incretin therapies | Daily route and lower ceiling reduce current ranking | Explains why it is secondary in Ana's Blueprint |
- Individual tolerance and adherence vary.
- Daily use can become a practical barrier.
- Maintenance after stopping still needs a plan.
- Comparative fit depends on access to newer agents.
Safety, side effects, and contraindications
- Nausea
- Vomiting or diarrhea
- Constipation
- Reflux or abdominal discomfort
- Reduced appetite
- Pancreatitis caution
- Gallbladder problems
- Dehydration during GI symptoms
- Acute kidney injury risk during volume depletion
- Heart rate increase
- Pulmonary aspiration risk disclosure before general anesthesia or deep sedation
- Lean-mass loss if intake drops too quickly
- Daily adherence fatigue
- Personal or family history of medullary thyroid carcinoma
- MEN2
- Prior pancreatitis requires review
- Severe gastroparesis or severe gastrointestinal disease requires review
- Pregnancy or lactation
- Eating disorder history requires caution
- Glucose-lowering medication requires monitoring
For Ana, liraglutide's main limitation is not relevance of the pathway; it is whether daily use offers enough advantage over weekly GLP-1 or dual-agonist options after prior category exposure.
Reference protocol
FDA label anchor: Saxenda chronic weight-management labeling is the primary anchor. Victoza is a diabetes label and is not automatically the same indication.
- Victoza used as if it were the Saxenda weight-management label
- Compounded liraglutide or non-branded vials
- Research-only GLP-1 products
- Weekly GLP-1 labels such as Wegovy
- Community dose charts
| Item | Reference |
|---|---|
| Label ladder | Saxenda labeling describes daily escalation through 0.6 mg, 1.2 mg, 1.8 mg, and 2.4 mg to adult maintenance at 3 mg daily; this is label context, not a personal dose. |
| Application footprint | Daily injection framing: about 30 administrations per month. |
| Route | Subcutaneous injection in the Saxenda/Victoza-style label context. |
| Time to maintenance | Adult maintenance is reached after weekly daily-dose escalation if tolerated. |
| Decision points | Daily adherence, GI tolerance, appetite response, glucose markers, nutrition adequacy, body composition, and access. |
- The first weeks are about daily routine and GI tolerance.
- Daily use makes adherence part of the efficacy question.
- The label uses a daily dose-escalation pathway.
- Tolerance and persistent symptoms should drive reassessment instead of automatic continuation.
- Track appetite, food noise, GI symptoms, hydration, protein intake, and training continuity.
- Daily burden should be considered alongside weight response.
- Maintenance is a daily long-term commitment in the Saxenda context.
- Lower practical ceiling and daily burden explain why it often ranks below weekly incretins.
- Plateau should trigger review of adherence, intake, dose history, symptoms, and access.
- Switching to weekly incretins may be a practical comparison, not an automatic next step.
| Item | Reference |
|---|---|
| Reference framing | Daily low-dose start with gradual escalation |
| Frequency | Once daily |
| Route | Subcutaneous |
| Decision points | GI tolerance, adherence, appetite response, glucose markers, and body composition |
| Use-case | Established GLP-1 option when daily dosing is acceptable |
- Can the user sustain daily administration?
- Is the current GI profile compatible with escalation or maintenance?
- Are contraindications and glucose-lowering medications reviewed?
- Does daily liraglutide offer enough advantage over weekly options?
- Is plateau caused by biology, adherence burden, or access friction?
- Escalation timing if tolerability requires review.
- Whether daily dosing is acceptable or creates too much friction.
- Follow-up cadence based on glucose, GI symptoms, and body composition.
- Role as fallback, comparator, or primary option depending on access.
- Saxenda versus Victoza indication boundaries.
- Contraindication review for MTC/MEN2, pancreatitis history, pregnancy, and serious hypersensitivity.
- Treating daily liraglutide as interchangeable with weekly semaglutide or tirzepatide.
- Combining with other incretins without professional review.
- Using vial-unit conversions or community charts.
Administration should follow the exact Saxenda or Victoza product label. The Blueprint does not convert daily pen dosing into non-label vial instructions.
- Confirm product and indication before interpreting dose language.
- Daily use creates more repeated handling than weekly options.
- Use label-specific storage, device, and missed-dose instructions.
Liraglutide maintenance is less about a dramatic ceiling and more about whether a daily GLP-1 remains sustainable.
- Review appetite control, daily adherence, GI tolerance, and access before continuing long term.
- Plan for weight-maintenance behaviors before stopping, switching, or pausing.
- If daily burden is the limiting factor, the comparison may shift toward weekly label anchors.
| Question | Reference answer |
|---|---|
| How many applications per month? | Daily framing is about 30 administrations per month. |
| Is this the same as semaglutide? | No. It shares GLP-1 biology but has different product labels, cadence, and practical burden. |
| Why does it rank lower? | Daily administration and lower modern category ceiling reduce practical fit for many Weight Loss profiles. |
| Can it be combined with another GLP-1? | That belongs in professional review; overlapping incretin pathways should not be improvised. |
| Is there a universal off-ramp? | No. Maintenance planning should be individualized around appetite, weight trend, and nutrition/training continuity. |
Educational reference based on public prescribing patterns and literature. This is not a prescription.
- Do not choose daily dosing without considering adherence burden.
- Do not ignore persistent GI symptoms.
- Do not combine with other GLP-1 or incretin agents without professional review.
- Do not treat scale loss as success if lean mass is falling.
Monitoring and labs
- Weight and waist circumference
- Body composition if available
- Fasting glucose and HbA1c
- Lipid profile
- Kidney and liver function
- Contraindication and medication review
- Daily adherence
- GI tolerance
- Hydration
- Protein intake
- Training continuity
- Glucose response
- Plateau pattern
- Lean mass
- Appetite control
- Routine burden
- Long-term access
The monitoring question is whether a daily GLP-1 routine creates enough benefit to justify its friction.
Regulatory status & study stage
Liraglutide is an approved GLP-1 drug in specific branded indications, including chronic weight management and type 2 diabetes.
| Item | Status | How to read it |
|---|---|---|
| Saxenda | FDA approved for chronic weight management | This is the weight-management branded pathway for liraglutide. |
| Victoza | FDA approved for type 2 diabetes | Same molecule family context, different branded indication. |
| Study stage | Approved with mature category evidence | Established, but often less competitive than newer weekly incretins. |
- Approved medication in specific indications.
- Clinical evidence is established but no longer category-leading.
- Useful as comparator or fallback in modern Weight Loss ranking.
- Branded prescription pathways exist.
- Daily administration changes practical adherence.
- Compounded or research-only products should not be treated as equivalent.
Approval is product- and indication-specific. It does not make all liraglutide sources equivalent.
Stacking and synergies
Liraglutide stacking should be interpreted through GLP-1 redundancy and daily-adherence burden.
- Liraglutide plus protein and resistance training.
- Liraglutide plus body-composition monitoring.
- Liraglutide plus adherence tracking if daily routine is chosen.
- Liraglutide plus semaglutide, tirzepatide, or another incretin without professional review.
- Liraglutide plus another appetite suppressant to compensate for low response.
- Insulin or sulfonylurea use
- Other incretin agents
- Pancreatitis or gallbladder history
- Aggressive weight-loss protocols
Do not layer daily and weekly incretin logic casually; overlapping pathways increase confusion and risk.
Genetic variable
Liraglutide shares the GLP-1 genetic context of the category. Appetite, obesity-risk, and glycemic-risk genes may influence expectations but do not determine fit alone.
- Metabolic-risk genetics can shape baseline context.
- GLP-1 response may eventually be refined by receptor and appetite-pathway genetics.
- No single variant should decide liraglutide use.
For liraglutide, adherence and tolerance usually matter more than genetics in the current Blueprint.
Real-world reports
- Appetite reduction
- Daily injection fatigue
- GI effects during escalation
- Less dramatic expectations than newer weekly agents
- Use when newer options are unavailable
- Daily routine burden
- Cost
- GI tolerance
- Lower perceived efficacy
- Switching to weekly alternatives
- Reports often compare liraglutide against newer GLP-1 options.
- Adherence is part of efficacy in real life.
- Anecdotes should not replace clinical evidence or access review.
Final personalized interpretation
For Ana, liraglutide is not irrelevant. The GLP-1 pathway matches appetite pressure and metabolic context, and its approved status gives it more maturity than research-only compounds.
The problem is comparative fit. Ana already has semaglutide exposure in the profile, and daily liraglutide is less attractive when weekly semaglutide and tirzepatide sit above it on evidence, convenience, and likely ceiling.
If access or tolerability made weekly options impractical, liraglutide could still be part of the conversation. But it does not solve the core ranking question better than the higher-ranked incretin options.
Its role in Ana's Blueprint is therefore as a clinically familiar backup or comparator, not as the lead recommendation candidate.
The practical read is secondary fit: relevant biology, approved pathway, but lower leverage for Ana's current Weight Loss profile.