Larazotide
Tight-junction comparator for permeability literacy, not a current leaky-gut solution.
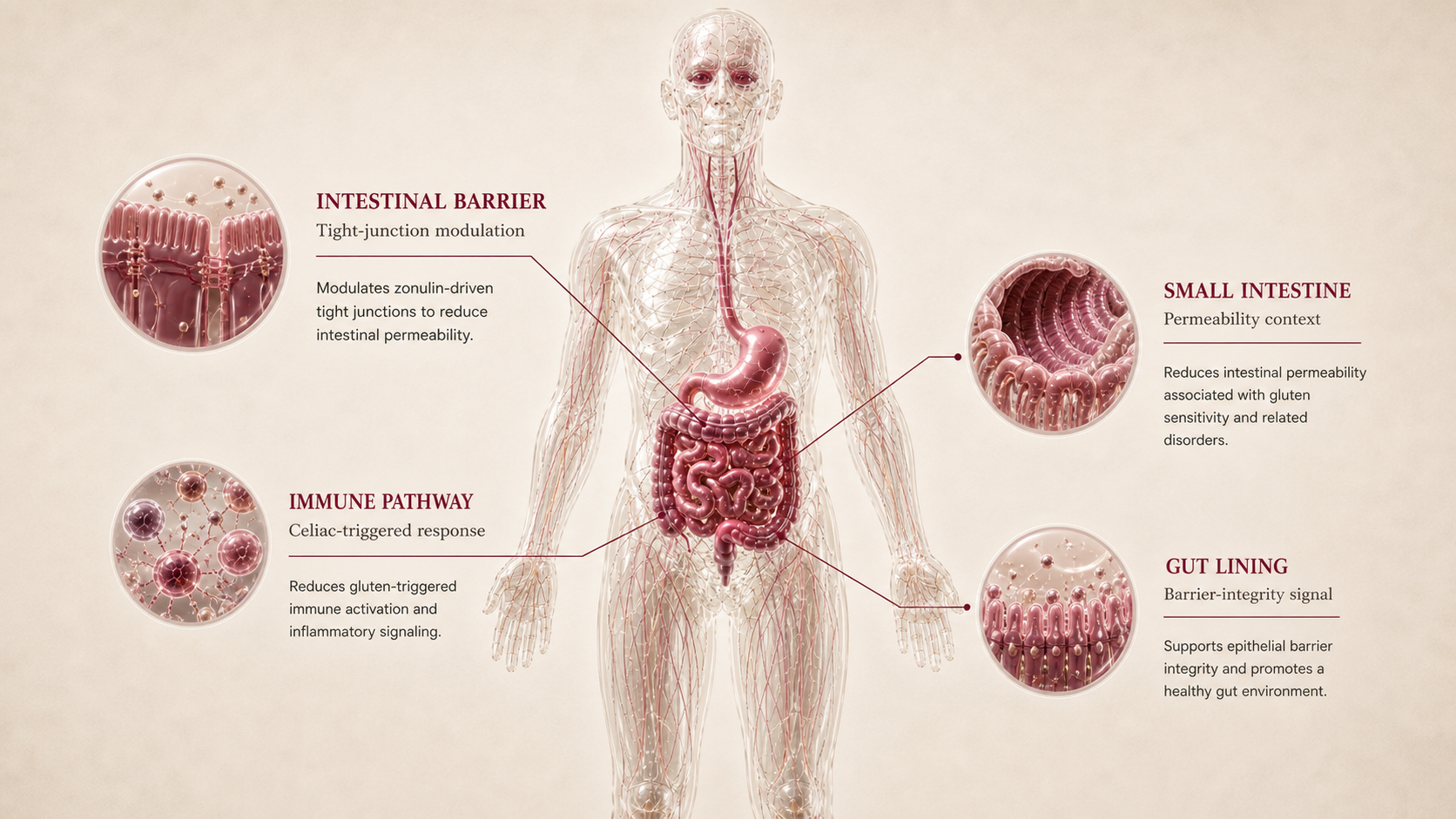
Larazotide in Gut Health is framed as tight-junction / intestinal permeability modulation. The report separates mechanism, human gut-health outcome evidence, and regulatory status.
Larazotide helps explain permeability and celiac tight-junction comparator. For Ana, it is evaluated against bloating, food triggers, suspected permeability, anxiety-linked gut unpredictability, Hashimoto, PCOS, metformin use, and lack of a confirmed IBD/SIBO diagnosis.
Why it may make sense for you
For Ana, Larazotide appears because the Gut Health profile combines persistent bloating, multiple food triggers, suspected permeability, anxiety around intestinal unpredictability, Hashimoto, PCOS, metformin use, and no robust formal GI diagnosis.
| Signal | Interpretation |
|---|---|
| Primary symptom pattern | Constant bloating and food-triggered symptoms |
| Barrier question | Suspected leaky gut / permeability |
| Inflammatory context | Hashimoto, PCOS, low-grade inflammation |
| Gut-brain context | Anxiety linked to intestinal unpredictability |
| Diagnostic boundary | No confirmed IBD, SIBO, celiac disease, or short bowel syndrome |
- Ana suspects permeability and reports gluten as one trigger, making the tight-junction concept educationally relevant.
- The dossier helps separate barrier, inflammation, motility, dysbiosis, and regulated GLP-2 categories.
- Ana has enough gut-context signals for education to be useful.
- No confirmed celiac diagnosis and no approved therapy status keep it below the more relevant barrier/inflammation candidates.
- Food triggers and bloating can reflect intolerance, celiac disease, IBS, SIBO, medication effects, reflux, thyroid context, or inflammatory disease.
- Red flags should move the conversation to medical evaluation, not peptide matching.
How it works
Larazotide is discussed as a tight-junction regulator intended to reduce gluten-triggered intestinal permeability in celiac disease research. In this report, it clarifies the difference between barrier concepts and practical availability.
| Pathway | Practical effect |
|---|---|
| Mechanistic evidence | Tight-junction / intestinal permeability modulation. |
| Human gut-health outcome evidence | Human research focused on celiac disease; the broader leaky-gut translation remains uncertain, and phase 3 did not establish a stable approved path. |
| Regulatory / label evidence | Larazotide is not approved as a general gut-health therapy and should be read as a permeability comparator. |
| Ana relevance | Permeability and celiac tight-junction comparator. |
Larazotide is useful for understanding one gut pathway, but a pathway is not the same as diagnosis, treatment, or a protocol.
What the evidence shows
Larazotide is framed through three evidence layers: mechanism, human gut-health outcomes, and regulatory/label status. Peptivius keeps these separate so gut-health marketing does not turn a plausible pathway into a treatment claim.
| Study | Population | Key result | How to read it |
|---|---|---|---|
| Mechanistic evidence | Tight-junction / intestinal permeability modulation. | Larazotide is discussed as a tight-junction regulator intended to reduce gluten-triggered intestinal permeability in celiac disease research. In this report, it clarifies the difference between barrier concepts and practical availability. | Explains why the peptide appears in Gut Health discussions. |
| Human gut-health outcome evidence | Outcome translation | Human research focused on celiac disease; the broader leaky-gut translation remains uncertain, and phase 3 did not establish a stable approved path. | Determines how far the claim can go. |
| Regulatory / label evidence | Phase 3 | Larazotide is not approved as a general gut-health therapy and should be read as a permeability comparator. | Defines practical boundary and approved-context status. |
- Whether the user's symptoms are IBS, IBD, SIBO, reflux, intolerance, celiac disease, medication-related, thyroid-linked, or another pattern.
- Whether human evidence supports the same claim being discussed in forums.
- Whether product identity, route, formulation, or source quality changes the risk profile.
Safety, side effects, and contraindications
- Gut symptom attribution can be unclear.
- Route/formulation uncertainty can change interpretation.
- Placebo, diet changes, and co-interventions can dominate perceived effects.
- Not approved, not a leaky-gut cure, and development limitations matter.
- Blood in stool, anemia, fever, nocturnal diarrhea, progressive pain, persistent vomiting, dysphagia, dehydration, or unintentional weight loss require evaluation.
- Active IBD, suspected infection, immunosuppression, chronic corticosteroid use, pregnancy, or cancer history need professional review.
- Research-only, compounded, and grey-market products are not equivalent to approved gut medications.
- Red-flag GI symptoms without evaluation.
- Known or suspected obstruction, severe dehydration, acute abdomen, or rapidly worsening abdominal pain.
- Active serious infection or uncontrolled inflammatory disease without clinician oversight.
- Pregnancy or lactation without medical supervision.
- Using a peptide to delay diagnosis or standard care.
For Ana, Larazotide should be read through the fact that symptoms are persistent but not yet diagnostically settled. The priority is pattern clarity, food-trigger mapping, labs/testing when appropriate, and red-flag screening.
Reference protocol
Pipeline comparator / development context: Larazotide celiac disease tight-junction trial and discontinued phase 3 context.
- Diagnosis, medical evaluation, endoscopy, stool testing, breath testing, celiac workup, or gastroenterology care.
- A personal protocol, dose plan, stack, supplier path, or treatment recommendation.
- Community protocols, compounded blends, or research-only products marketed as gut-healing solutions.
| Item | Reference |
|---|---|
| Reference frame | Pipeline/discontinued permeability comparator |
| Gut role | Permeability and celiac tight-junction comparator. |
| Evidence layer | Studied in celiac disease and permeability contexts, but phase 3 development did not create an approved practical option. |
| Practical readiness | Low; educational comparator rather than current consumer Gut Health path. |
| Not a protocol | No dose, timing, cycle, vial, syringe, unit, or supplier guidance. |
- Clarify the symptom pattern, food triggers, medication context, prior workup, and red flags.
- Separate barrier, inflammation, motility, reflux, dysbiosis, celiac, and malabsorption hypotheses.
- Use professional review when symptoms are severe, progressive, inflammatory, or unexplained.
- Read Larazotide as pipeline/discontinued permeability comparator, not as a consumer use plan.
- Keep mechanism, human outcome evidence, and regulatory status separated.
- Avoid treating gut discomfort as one universal category.
- Track symptoms, stool pattern, food tolerance, reflux, energy, weight change, hydration, and new red flags.
- Escalate evaluation rather than peptide experimentation when alarm features appear.
- Treat stopping, deferring, or seeking workup as a valid conclusion.
| Item | Reference |
|---|---|
| Reference mode | Pipeline/discontinued permeability comparator |
| Primary anchor | Larazotide celiac disease tight-junction trial and discontinued phase 3 context. |
| Route label | Oral as category descriptor, not instruction. |
| Timing | No consumer protocol timeline. |
| Decision points | Diagnosis, red flags, food triggers, medications, labs/testing, and professional review. |
- Is this barrier, inflammation, motility, reflux, dysbiosis, celiac, or malabsorption?
- Are red flags present?
- Has a clinician ruled out conditions that should not be self-managed?
- Would a peptide obscure the diagnosis or reduce clarity?
- Is the evidence layer being confused with a treatment plan?
- Which gut hypothesis is most relevant.
- Which tests or clinical review are needed.
- How food triggers, stress, medication, and thyroid/metabolic context change the interpretation.
- Red-flag triage.
- Approved indication boundaries.
- The difference between research-only peptides and approved medications.
- Avoidance of dose conversions, cycles, blends, and supplier guidance.
Administration is included only as category literacy. The report does not instruct the reader to administer a gut peptide.
- Route labels in the report are descriptive, not recommendations.
- Gut peptides are especially easy to over-market because symptoms are common and nonspecific.
- Product identity, route, formulation, and source quality can dominate safety interpretation.
Gut Health maintenance is about diagnostic clarity, symptom stability, sustainable diet, and professional care when needed.
- Track food tolerance and symptom patterns rather than chasing a peptide timeline.
- Revisit labs, stool markers, or gastroenterology evaluation if symptoms persist.
- Do not use peptides to delay care for inflammatory, bleeding, obstructive, or malabsorptive patterns.
| Question | Reference answer |
|---|---|
| Is this a gut protocol? | No. It is mechanism and evidence literacy. |
| Can this replace a gastroenterologist? | No. Diagnosis and red-flag evaluation come first. |
| Can I treat SIBO, IBD, or leaky gut with this? | The report does not make that recommendation. |
| Why include regulatory anchors? | They show what approved gut peptide evidence looks like, and where the boundaries are. |
Reference context only. This dossier does not provide a dose, schedule, duration, cycle, vial conversion, syringe unit, supplier path, or personal protocol.
- Do not treat gut discomfort as one universal peptide problem.
- Do not use peptide matching to delay evaluation of red flags.
- Do not infer a stack, blend, or protocol from mechanism overlap.
- Do not treat research-only products as equivalent to approved medications.
Monitoring and labs
- Bowel pattern, stool frequency, urgency, constipation, diarrhea, and nocturnal symptoms.
- Pain, bloating, reflux, nausea, vomiting, hydration, and weight trend.
- Food triggers: gluten, lactose, FODMAPs, meal timing, alcohol, caffeine, and supplements.
- Medication context: metformin tolerance, thyroid medication, acid suppression, NSAIDs, antibiotics, and probiotics.
- Prior workup: celiac testing, stool tests, SIBO breath testing, endoscopy history, fecal calprotectin if applicable.
- CBC, ferritin, B12, vitamin D, inflammatory markers, and thyroid/metabolic context when relevant.
- Symptom frequency and intensity.
- Food tolerance and trigger consistency.
- Diarrhea, constipation, reflux, pain at night, hydration, energy, and weight.
- New red flags or symptom progression.
- Whether a structured diet or clinical evaluation has clarified the pattern.
- Stable symptom pattern and known triggers.
- Sustainable diet strategy rather than endless restriction.
- Need for gastroenterology follow-up or further testing.
- Response to conventional care when indicated.
- Relationship with sleep, stress, anxiety, and gut-brain patterns.
The goal is not just reducing discomfort. It is understanding the pattern, identifying red flags, avoiding overclaiming, and building a safe strategy.
Regulatory status & study stage
Larazotide is not approved as a general gut-health therapy and should be read as a permeability comparator.
| Item | Status | How to read it |
|---|---|---|
| Status | Phase 3 | Interpret only inside the stated anchor. |
| Gut indication | Permeability and celiac tight-junction comparator. | Not all gut roles are clinical indications. |
| Readiness | Low; educational comparator rather than current consumer Gut Health path. | Practical readiness is separate from mechanism interest. |
- Human research focused on celiac disease; the broader leaky-gut translation remains uncertain, and phase 3 did not establish a stable approved path.
- Gut symptoms require diagnostic context before outcome claims can be interpreted.
- Low; educational comparator rather than current consumer Gut Health path.
- No supplier, dose, or protocol guidance is provided.
This dossier does not convert label, trial, research, or comparator context into consumer instructions.
Stacking and synergies
Larazotide may appear in gut-healing stacks online, but Peptivius keeps combination literacy at the niche level. This dossier evaluates the individual peptide.
- Symptom journal, food-trigger mapping, hydration, and bowel-pattern tracking.
- Clinician-guided testing when celiac disease, IBD, SIBO, malabsorption, or reflux complications are possible.
- Sleep and stress support when gut-brain patterns are present.
- Multiple gut peptides layered without a diagnosis.
- Barrier plus antimicrobial plus immune peptides used as a broad gut-healing blend.
- Adding peptides while ignoring metformin tolerance, thyroid context, or dietary triggers.
- Blood, anemia, weight loss, nocturnal diarrhea, severe pain, vomiting, or dysphagia.
- Known IBD, celiac disease, immunosuppression, chronic steroid use, or suspected infection.
- Any antimicrobial peptide or GLP-2 class discussion.
A gut stack can reduce clarity. If symptoms change, it becomes harder to know whether food, medication, infection, inflammation, placebo, or a peptide caused the change.
Genetic variable
Larazotide has no validated consumer genetic response engine in Peptivius today. The genes below are pathway literacy only for barrier, immune, motility, celiac, or microbiome-related interpretation.
- No validated genotype determines whether this peptide is appropriate for Ana.
- Pathway genes may help explain barrier, immune, motility, or celiac-risk differences.
- No SNP should convert gut symptoms into a peptide recommendation.
Future DNA layers may refine gut interpretation, but Slice 1 does not personalize gut peptides from genotype.
Real-world reports
- Gut-health anecdotes often mix peptides with elimination diets, probiotics, antibiotics, supplements, and stress changes.
- Users frequently report nonspecific symptoms such as bloating, reflux, constipation, or food reactivity without a confirmed diagnosis.
- Research-only product quality and route claims are recurring concerns.
- New red flags or symptom progression.
- Unclear diagnosis or worsening GI symptoms.
- Concern that a peptide is masking the need for standard evaluation.
- Anecdotes can reveal what users ask, but they do not prove gut-health efficacy.
- The strongest interpretation comes from diagnosis, symptom tracking, labs/testing, and response to conventional foundations.
- Blend marketing should be decomposed into component mechanisms.
Final personalized interpretation
For Ana, Larazotide is best read through a diagnostic-clarity lens. The profile has meaningful gut signals: persistent bloating, suspected permeability, gluten/lactose/FODMAP triggers, anxiety around unpredictability, Hashimoto, PCOS, metformin exposure, and low-grade inflammatory context.
That does not mean the problem is automatically leaky gut, SIBO, IBD, or reflux. It means the report should separate barrier, inflammation, gut-brain, motility, dysbiosis, celiac/permeability, and regulated GLP-2 concepts before any peptide receives too much credit.
Larazotide is useful because it explains one part of that map. It does not replace gastroenterology review, red-flag triage, stool/lab testing when appropriate, structured diet work, or medication review.
For Ana, Larazotide should be read as Gut Health education, not a protocol or treatment instruction.