KPV
The anti-inflammatory and gut-immune context peptide in Recovery & Healing, not a primary structural repair tool.
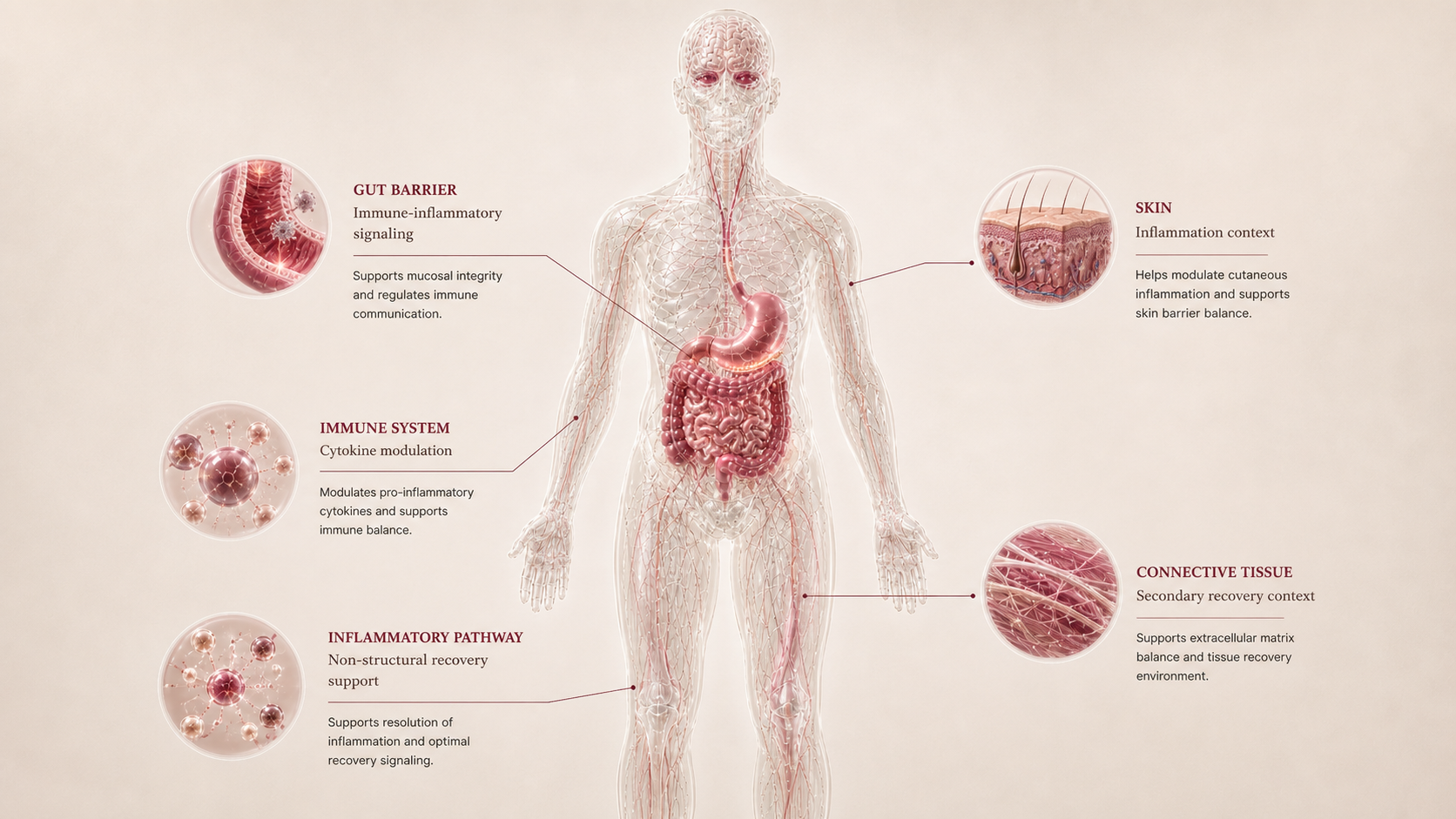
Melanocortin-derived tripeptide, Lys-Pro-Val, discussed in anti-inflammatory, gut, skin, and immune-modulation research.
KPV belongs in Recovery & Healing because some recovery problems are inflammatory rather than purely mechanical. It is not framed as a tendon, ligament, or cartilage repair peptide. Its role is to help the reader separate inflammation-driven recovery from structural injury recovery.
Why it may make sense for you
For Ana, KPV is included because recovery can be shaped by inflammation, gut context, and autoimmune background. It ranks below structural-recovery candidates because the main pain point is still a chronic knee tendon issue. Data confidence is Medium: inflammatory context is visible, but clearer labs, diagnosis, symptom pattern, and rehab history would improve interpretation.
| Signal | Interpretation |
|---|---|
| Recovery signal | Inflammatory and gut-immune context |
| Best role | Inflammation literacy rather than tissue repair |
| Data confidence | Medium - autoimmune/gut context is visible, but inflammatory markers, diagnosis detail, symptom pattern, imaging, and rehab history remain incomplete. |
| Lower-fit reason | Not a primary mechanical injury peptide |
| Main caution | Do not bypass immune or gut medical evaluation |
- Relevant to inflammation-driven recovery questions.
- Can connect gut, skin, immune, and systemic recovery themes.
- Useful contrast against BPC-157/TB-500 structural narratives.
- Does not solve loading mechanics.
- Autoimmune and gut symptoms need medical context.
- Evidence is preclinical-heavy for many claims.
How it works
KPV is a tripeptide derived from the C-terminal sequence of alpha-MSH. It is discussed for anti-inflammatory signaling, gut-immune modulation, and cytokine pathway effects. In Recovery & Healing, that means inflammation context, not direct structural repair.
| Pathway | Practical effect |
|---|---|
| Melanocortin context | KPV derives from alpha-MSH anti-inflammatory biology. |
| Gut immune | Murine colitis models explain why gut-recovery claims appear. |
| Cytokine signaling | Anti-inflammatory pathway discussion can frame systemic recovery. |
| Mechanical boundary | Tendon and ligament recovery still require diagnosis and loading. |
KPV is the inflammation branch of the Recovery map, not the tendon-repair branch.
What the evidence shows
KPV has three evidence layers: mechanistic evidence is anti-inflammatory and gut-immune but mostly preclinical; human outcome evidence is low for Recovery & Healing; regulatory/label evidence is absent for structural repair or broad recovery.
| Study | Population | Key result | How to read it |
|---|---|---|---|
| Mechanistic evidence | Melanocortin-derived anti-inflammatory and gut-immune models | KPV shows anti-inflammatory effects in murine colitis and intestinal inflammation research | Mostly preclinical; good for inflammation literacy, not tendon repair. |
| Human outcome evidence | Recovery and injury context | No mature human recovery or structural-injury outcome package is established here | Low for Recovery & Healing. |
| Regulatory / label evidence | FDA safety-risk / withdrawn nomination context | FDA notes lack of identified human exposure data for KPV in nominated context | No approved recovery, tendon, IBD, or structural-repair label. |
- Human recovery and injury evidence is not mature.
- Best indication, route, and monitoring are not standardized in this report.
- Autoimmune and IBD contexts require medical oversight.
- Blend evidence is not equivalent to KPV evidence.
Safety, side effects, and contraindications
- Tolerability is not well standardized across human recovery contexts.
- Gut, skin, or immune symptoms may be difficult to attribute.
- Blend use can hide the actual driver of benefit or side effects.
- Autoimmune disease, IBD symptoms, infection, and immunosuppression require professional review.
- FDA safety-risk materials note lack of identified human exposure data.
- Mechanical injuries should not be reframed as immune problems without evidence.
- Severe gut symptoms, bleeding, fever, infection signs, or unexplained abdominal pain without medical evaluation.
- Active autoimmune flare or immunosuppressive medication context without clinician review.
- Pregnancy or lactation without professional review.
- Use inside a multi-peptide blend when attribution is needed.
- Fever, infection signs, neurologic symptoms, progressive night pain, suspected fracture, severe unexplained pain, or mechanical injury worsening despite rest.
For Ana, KPV should be read as inflammatory-context education because Hashimoto/PCOS/gut context exists, but the knee issue remains primarily mechanical until proven otherwise.
Reference protocol
Variable clinical context: KPV is anchored to melanocortin-derived anti-inflammatory and gut-immune research, not to an approved structural-repair label.
- BPC-157 or TB-500 tissue-repair framing
- KLOW-like blends treated as a single evidence-backed product
- IBD or autoimmune treatment plans
- Mechanical injury protocols
- Research products treated as standardized medication
| Item | Reference |
|---|---|
| Reference | Anti-inflammatory, gut-immune, and skin-barrier research context; not primary tendon repair. |
| Route/frequency | No standardized recovery schedule is published here. |
| Application footprint | Depends on whether the driver is gut, skin, systemic inflammation, or mechanical injury. |
| Decision frame | Inflammatory pattern, diagnosis, immune history, gut symptoms, skin context, and professional review. |
- Clarify whether the recovery problem is inflammation-driven, gut-immune related, skin-barrier related, or mechanical tissue damage.
- KPV is not read as a primary repair tool for tendons or ligaments.
- Autoimmune disease, IBD symptoms, infection, immunosuppression, and medication context change the conversation.
- Do not use peptide framing to bypass diagnostic workup for inflammatory disease.
- Track inflammatory symptoms, gut/skin pattern, training tolerance, and adverse effects separately.
- If mixed into blends, causality becomes weak.
- Persistent gut bleeding, severe pain, fever, infection signs, or autoimmune flare symptoms need professional care.
- Mechanical pain that does not improve should return to injury diagnosis and rehab logic.
| Item | Reference |
|---|---|
| Source anchor | Melanocortin-derived anti-inflammatory and gut-immune research plus FDA safety-risk context. |
| Protocol status | No universal recovery schedule, route conversion, or application count. |
| Main dependency | Inflammatory driver, diagnosis, immune history, gut/skin context, and professional review. |
| Blend boundary | KPV inside KLOW-like blends is not treated as a single evidence-backed product. |
- Is inflammation the driver, or is this primarily mechanical tissue damage?
- Are gut, skin, autoimmune, infection, or medication factors present?
- Is the claim based on murine colitis research or human clinical evidence?
- Is KPV being hidden inside a blend where attribution is impossible?
- Would medical workup matter more than peptide selection?
- Whether the emphasis is gut-immune, skin inflammation, or systemic inflammation context.
- How clinicians interpret preclinical colitis models versus real-world inflammatory complaints.
- Monitoring focus based on symptoms and medications.
- The absence of an approved recovery or IBD treatment label.
- FDA safety-risk framing around lack of identified human exposure data.
- Autoimmune, infection, pregnancy, immunosuppressive medication, and IBD red-flag review.
- Using KPV as if it repairs mechanical tendon damage.
- Treating KLOW-like blends as a single studied product.
KPV administration language should stay tied to source context. This report does not turn animal, gut, skin, or blend discussion into protocol instructions.
- Separate gut, skin, systemic inflammation, and mechanical injury claims.
- Do not infer human route or frequency from animal models.
- Treat immune and inflammatory disease symptoms as medical context, not lifestyle noise.
- Avoid blends when the goal is to understand whether KPV itself matters.
KPV maintenance is a question of inflammatory-driver clarity, not a universal recovery cycle.
- If symptoms are gut or immune related, diagnosis and medical monitoring matter.
- If pain is mechanical, rehab remains the central recovery path.
- If benefit is unclear, adding BPC-157, TB-500, or GHK-Cu can make interpretation worse.
| Question | Reference answer |
|---|---|
| Is KPV a tendon-healing peptide? | No. It is better framed as anti-inflammatory and gut-immune context. |
| Can KPV replace IBD or autoimmune care? | No. Gut bleeding, severe symptoms, infection, or autoimmune activity require medical evaluation. |
| Why is it in Recovery? | Some recovery problems are inflammatory rather than purely structural. KPV helps map that branch. |
| Is a KLOW-like blend the same as KPV evidence? | No. A blend combines multiple compounds and weakens attribution. |
Educational reference only. KPV is not presented as a protocol for inflammatory disease or injury repair.
- Do not use KPV as a tendon or ligament cure.
- Do not substitute it for IBD or autoimmune medical care.
- Do not infer human recovery protocols from animal models.
- Do not hide KPV inside blends when attribution matters.
Monitoring and labs
- Clarify diagnosis, injury type, injury age, location, imaging status, rehab plan, and current load-management strategy.
- Record pain at rest, pain during load, pain 24 hours after training, range of motion, strength, swelling, and training tolerance.
- Document return-to-run, return-to-squat, or return-to-sport markers when relevant.
- Record sleep impact, protein/nutrition context, rehab adherence, and medication changes.
- Review medications, procedures, autoimmune history, cancer history, pregnancy context, and tested-sport status.
- Track function, pain at rest, pain under load, next-day pain, training load, swelling, local irritation, systemic symptoms, and whether rehab tolerance actually improves.
- Separate normal loading adaptation from a peptide-attributed effect.
- Pause interpretation if multiple new compounds or blends were introduced together.
- Escalate medical review if new red-flag symptoms appear.
- Keep progressive loading, sleep, protein adequacy, and recurrence prevention as the foundation.
- Reassess if pain returns, function stalls, or the compound becomes a substitute for diagnosis or rehab.
- Use functional milestones rather than calendar promises to judge return-to-run, return-to-squat, or return-to-sport readiness.
- Treat stopping as an interpretation checkpoint, not as a universal taper.
For KPV, monitoring emphasizes inflammatory symptoms, gut/skin context, medication review, and whether the injury is actually mechanical.
Regulatory status & study stage
KPV is best read as research-sensitive anti-inflammatory and gut-immune context. It is not approved as a general Recovery & Healing therapy.
| Item | Status | How to read it |
|---|---|---|
| FDA label | No approved recovery label | No structural repair or IBD treatment label anchors this dossier. |
| FDA safety-risk page | Compounding concern | FDA notes no identified human exposure data for KPV in the nominated context. |
| Evidence stage | Preclinical-heavy | Murine colitis and gut-immune studies support mechanism, not broad human recovery use. |
- Anti-inflammatory research is the main evidence lane.
- Human recovery translation remains limited.
- Inflammatory disease claims require professional context.
- Research-only products are not equivalent to approved care.
- Blends obscure KPV-specific interpretation.
- Medical evaluation comes first for significant gut or immune symptoms.
The dossier keeps KPV in its anti-inflammatory lane.
Stacking and synergies
KPV appears in multi-peptide healing blends, but Peptivius evaluates it individually and places blend literacy in the final niche map.
- Medical evaluation for gut, skin, or immune symptoms.
- Rehab and loading if the recovery issue is mechanical.
- Nutrition, sleep, and stress context for inflammatory recovery patterns.
- KPV plus KLOW-like blends when attribution is needed.
- KPV used to explain mechanical pain without inflammatory evidence.
- Multiple anti-inflammatory strategies without diagnosis.
- Autoimmune disease, IBD symptoms, infection, pregnancy, or immunosuppressive medication.
- Severe or unexplained gut symptoms.
- Use inside multi-peptide blends.
Do not turn inflammation biology into a treatment plan for undiagnosed disease.
Genetic variable
No validated consumer genetic marker predicts KPV response. Immune, inflammatory, gut-barrier, and cytokine genetics can provide general context only.
- No validated KPV response genotype.
- Inflammation and gut-transporter genetics can frame research hypotheses.
- No SNP should turn KPV into a treatment recommendation.
Genetics may explain inflammatory vulnerability, not KPV selection.
Real-world reports
- Users discuss gut inflammation, skin inflammation, and systemic inflammatory recovery.
- KPV appears inside all-in-one blends.
- Some users confuse anti-inflammatory context with structural healing.
- Gut or immune symptoms require medical evaluation.
- No obvious mechanical recovery improvement.
- Unclear blend attribution.
- Limited human evidence.
- Real-world discussion supports inclusion as an inflammation branch.
- It does not establish injury-repair efficacy.
- Medical red flags override peptide interest.
Final personalized interpretation
For Ana, KPV is relevant because the broader profile includes autoimmune and metabolic-inflammatory context. That matters for recovery interpretation.
It stays below BPC-157, TB-500, and GHK-Cu because the main Recovery problem is patellar tendinopathy, where structural loading and localized tissue context are more direct.
KPV becomes most useful if the recovery bottleneck looks inflammatory or gut-immune rather than mechanical.
For Ana, KPV is a secondary inflammation-context compound, not the lead healing peptide.