CagriSema
An emerging amylin-plus-GLP-1 combination that may shape the next wave of appetite biology.
Investigational fixed-dose combination concept pairing cagrilintide, an amylin analog, with semaglutide, a GLP-1 receptor agonist.
CagriSema is relevant because it combines two appetite-related pathways: GLP-1 and amylin. It is promising as a category signal, but current practical fit is limited by approval and access status.
Why it may make sense for you
For Ana, CagriSema is scientifically relevant because appetite biology is central to the profile, but it ranks lowest among the Weight Loss set because practical availability and regulatory maturity are less settled.
| Signal | Interpretation |
|---|---|
| Declared objective | Significant weight loss and appetite control |
| Mechanism relevance | GLP-1 plus amylin satiety framing |
| Practical limitation | Pipeline and access uncertainty |
| Comparison role | Future alternative to semaglutide-style therapy |
| Rank reason | Interesting category signal, not current practical lead |
- Directly relevant to food-noise and satiety biology.
- Useful to understand the category beyond GLP-1 alone.
- May matter in future if approved and accessible.
- Strong conceptual relevance to Ana's appetite pattern.
- Current status limits practical fit.
- Not equivalent to approved semaglutide or tirzepatide pathways.
- GI tolerance and low intake would require careful monitoring.
- Ana's current report should prioritize more mature options.
How it works
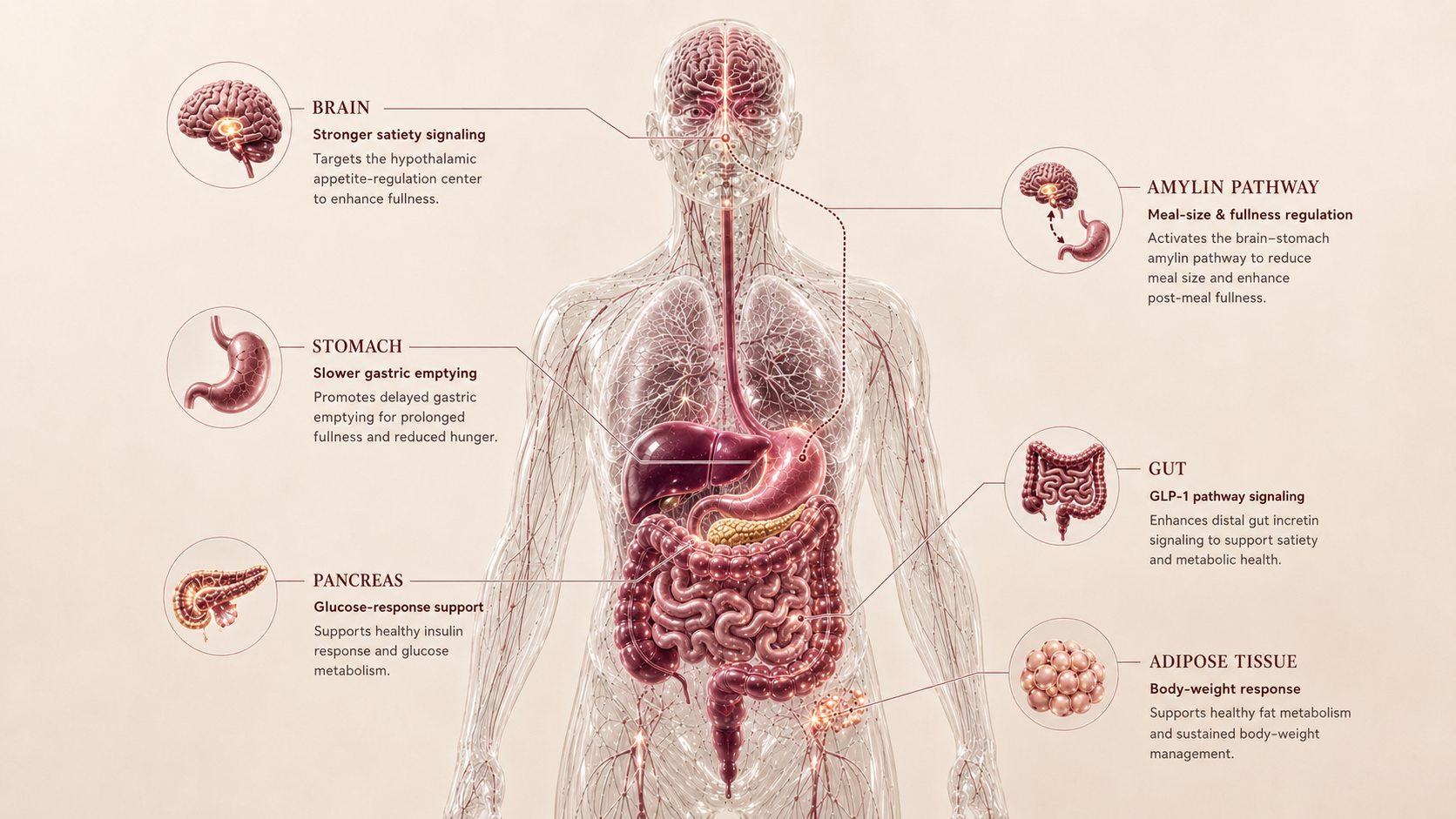
CagriSema combines GLP-1 signaling from semaglutide with amylin-pathway signaling from cagrilintide. GLP-1 supports satiety and glucose response, while amylin biology adds another meal-size and fullness signal.
| Pathway | Practical effect |
|---|---|
| GLP-1 | Satiety and glucose response |
| Amylin | Meal-size and fullness signaling |
| Gut-brain axis | Potentially stronger appetite regulation |
| Practical result | Future multi-pathway weight-loss strategy |
CagriSema is about adding another satiety signal to GLP-1, but the practical story is still developing.
What the evidence shows
CagriSema has strong category relevance because it tests whether GLP-1 plus amylin can outperform GLP-1 alone. The evidence is promising but still tied to clinical-development status.
| Study | Population | Key result | How to read it |
|---|---|---|---|
| Phase 3 obesity program | Adults with obesity or overweight | Combination approach under late-stage study | Important for future category direction |
| Cagrilintide + semaglutide studies | Weight-management populations | Dual-pathway appetite strategy | Explains why it matters beyond semaglutide alone |
| Category comparison | Incretin and appetite agents | Amylin pathway may broaden satiety biology | Useful as a pipeline comparator, not a settled access option |
- Final approval and label remain unsettled.
- Long-term real-world adherence is not mature.
- Tolerability relative to existing options needs practical context.
- Access and pricing are future-dependent.
Safety, side effects, and contraindications
- Nausea
- Vomiting or diarrhea
- Constipation
- Reduced appetite
- Injection-site discomfort
- GI burden from combined appetite pathways
- Low intake and protein adequacy
- Dehydration
- Lean-mass loss during rapid weight change
- Pipeline-stage uncertainty
- Regulatory and quality risk from attempts to recreate the combination outside approved or trial supply
- Professional review for thyroid cancer/MEN2 context
- Professional review for pancreatitis history
- Pregnancy or lactation
- Eating disorder history requires caution
- Glucose-lowering medication requires monitoring
For Ana, CagriSema's main caution is timing: the biology is relevant to food noise, but the current decision should favor options with clearer approval, access, and monitoring pathways.
Reference protocol
Pipeline combination anchor: CagriSema is anchored to phase 3 REDEFINE and ClinicalTrials.gov once-weekly combination-study context while regulatory review is unsettled.
- An approved CagriSema consumer label
- Semaglutide alone
- Cagrilintide alone
- A compounded cagrilintide-plus-semaglutide blend; FDA says cagrilintide cannot be used in compounding under federal law
- A community amylin/GLP-1 stack
| Item | Reference |
|---|---|
| Reference framing | Pipeline fixed-combination GLP-1 plus amylin context. |
| Studied cadence | Phase 3 records describe once-weekly subcutaneous combination exposure. |
| Dose context | REDEFINE obesity studies evaluate 2.4 mg / 2.4 mg combination framing; this is trial/NDA context, not a consumer protocol. |
| Time horizon | REDEFINE obesity studies use multi-month trial horizons such as 68 weeks. |
| Decision points | Regulatory status, combination tolerability, appetite suppression intensity, nutrition adequacy, and access legitimacy. |
- First question: is there a settled approved label and access pathway?
- Until approval is clear, this remains category education rather than current-use guidance.
- The combination is not the same as semaglutide alone.
- Component familiarity does not make a fixed combination automatically approved or interchangeable.
- Trial interpretation should include appetite response, GI tolerance, nutrition adequacy, and discontinuation patterns.
- Strong appetite suppression can become a nutrition problem if not monitored.
- Maintenance depends on future labeling, access, coverage, and post-market experience.
- The current Blueprint should treat it as a watch item rather than a current path.
- If the user needs an actionable option now, approved incretins are the comparison set.
- Do not self-build a combination stack to imitate a pipeline product.
| Item | Reference |
|---|---|
| Reference framing | Weekly fixed-combination clinical-development pathway |
| Route | Subcutaneous |
| Frequency | Weekly in development framing |
| Decision points | Approval status, tolerability, appetite response, nutrition adequacy, and access |
| Use-case | Future multi-pathway appetite control |
- Is the user treating a pipeline combination as an approved product?
- Is the access route legitimate or a research-only/compound blend?
- Is cagrilintide being treated as compoundable or interchangeable with an approved product?
- Does appetite suppression risk nutrition inadequacy?
- Are other incretin or amylin agents already being used?
- Would an approved single-agent or dual-agent label answer the current need more cleanly?
- Regulatory status as review progresses.
- Trial duration and comparator arms by study design.
- Future label language if approval occurs.
- How strongly the product fits once pricing, supply, and prescriber criteria are known.
- Treating CagriSema as already interchangeable with semaglutide.
- Building a do-it-yourself cagrilintide and semaglutide stack.
- Assuming cagrilintide can be compounded or sourced like an approved GLP-1 medication.
- Ignoring combination appetite suppression and nutrition adequacy.
- Combining with other incretins or appetite suppressants outside professional review.
- Assuming research-only blends match trial product quality or dosing.
Administration should stay in the trial and future-label frame. The Blueprint does not provide instructions for compounded or research-only attempts to recreate CagriSema.
- Read once-weekly exposure as study context until a label is settled.
- Do not infer syringe units, mixing steps, or component substitution from trial summaries.
- Do not treat compounded cagrilintide claims as equivalent to regulated CagriSema development.
- If approved, future product-specific label instructions would replace this pipeline framing.
Maintenance is not settled until there is a label and real access pathway. For now, the maintenance question is educational.
- Track the category because combination appetite biology may matter later.
- For current action, compare against approved options with established labels.
- Do not use pipeline excitement as a reason to bypass regulated access.
| Question | Reference answer |
|---|---|
| Is CagriSema approved here? | This Blueprint treats it as pipeline/regulatory-review context, not a settled current-use label. |
| Is it just semaglutide? | No. It combines semaglutide and cagrilintide biology in a fixed-combination trial context. |
| Can separate compounds recreate it? | No. A self-built stack is not equivalent to a regulated fixed-combination product. |
| How many applications? | Trial records describe once-weekly subcutaneous exposure, but this is not consumer access guidance. |
| Why include it? | It explains where appetite therapy is moving and why current approved options remain more actionable. |
Educational reference only. CagriSema is treated here as a clinical-development concept, not as a prescription or access recommendation.
- Do not treat CagriSema as equivalent to semaglutide alone.
- Do not treat pipeline products as approved medication.
- Do not combine additional incretins casually.
- Do not ignore nutrition adequacy when appetite is strongly suppressed.
Monitoring and labs
- Weight and waist circumference
- Body composition if available
- Fasting glucose and HbA1c
- Medication review
- Contraindication review
- Nutrition baseline
- GI tolerance
- Hydration
- Protein intake
- Appetite suppression intensity
- Energy and training continuity
- Lean mass
- Plateau pattern
- Metabolic labs
- Label/access updates
- Sustainability strategy
Monitoring should assume strong appetite biology but less mature practical experience than approved incretin options.
Regulatory status & study stage
CagriSema is best read as a late-stage clinical-development combination, not as an already settled FDA-approved combination pathway.
| Item | Status | How to read it |
|---|---|---|
| CagriSema | Phase 3 / investigational combination | Combines cagrilintide and semaglutide in a pipeline framing. |
| Semaglutide component | Approved in separate branded indications | Approval of semaglutide alone does not approve the combination. |
| Access | Not a settled routine prescription pathway | Practical use depends on future approval, label, availability, and coverage. |
- Late-stage clinical-development relevance.
- Strong category interest due to GLP-1 plus amylin biology.
- Not mature post-market evidence as a fixed combination.
- No routine approved combination pathway should be assumed.
- Compounded cagrilintide-plus-semaglutide should not be treated as a lawful or equivalent substitute.
- Research-only versions are not equivalent to approved medication.
- Current Blueprint use is mainly educational comparison.
Component familiarity does not make the fixed combination automatically approved or equivalent.
Stacking and synergies
CagriSema already combines appetite pathways, so stacking logic should be especially conservative.
- CagriSema plus protein and resistance training strategy in future approved context.
- CagriSema plus body-composition monitoring.
- CagriSema plus hydration and nutrition adequacy tracking.
- CagriSema plus semaglutide, tirzepatide, liraglutide, or another incretin.
- CagriSema plus another strong appetite suppressant without professional review.
- Glucose-lowering medication
- Other incretin agents
- Eating disorder history
- Aggressive weight-loss protocols
- Research-only sourcing scenario
Do not layer appetite-active compounds on top of a combination appetite therapy without a clear professional rationale.
Genetic variable
Future genetics may matter across GLP-1 response, amylin signaling, appetite regulation, and glycemic risk, but CagriSema-specific genetic interpretation is not mature.
- Appetite and glucose-risk genetics can frame baseline context.
- Amylin-pathway genetics may become relevant as the category matures.
- No current SNP should be used to predict CagriSema response.
Treat genetics as future expectation context, not as a current decision engine for CagriSema.
Real-world reports
- High interest because of dual-pathway appetite biology
- Expectation of stronger satiety than GLP-1 alone
- Questions about GI tolerability
- Confusion around semaglutide component vs combination
- Pipeline speculation
- Not approved as routine combination access
- GI concern
- Research-only risk
- Waiting for label and pricing
- Preference for approved options
- Most discussion is category expectation rather than mature use.
- Component familiarity does not equal combination maturity.
- Anecdotes should not replace regulatory status and clinical evidence.
Final personalized interpretation
For Ana, CagriSema is biologically relevant because the profile includes appetite pressure, food noise, metabolic context, and prior GLP-1 exposure. A GLP-1 plus amylin approach speaks directly to that landscape.
The reason it ranks last in the current Weight Loss list is practical maturity. Ana's profile needs a pathway that can be evaluated with clear access, monitoring, contraindication review, and continuity.
CagriSema is useful in this Blueprint because it shows where the field is heading: stronger multi-pathway satiety strategies. But right now, tirzepatide and semaglutide are more actionable comparison points.
The main caution is not that the biology is irrelevant. It is that a pipeline combination should not be treated like a settled treatment option.
For Ana, CagriSema is a future-category watch item, not the current lead match.